
Accurate Diagnosis of TMJ Pain and Dysfunction (Free Preview)
Quiz: When you have completed the learning material in this unit, you will be able to access its multiple-choice quiz by clicking on the link found at the bottom of this web page. You can attempt the quiz as many times as you need to achieve a pass mark of at least 80%.
Unit Credit: 2 Hours
How to Complete This Unit
The credit hours for this unit are allocated for progressing through the reading material, answering the questions posed, considering the reflection points, watching the videos, and completing the quiz. When you have completed the learning material in this unit, you will be able to access its multiple-choice quiz by clicking on the link found at the bottom of this web page. You can attempt the quiz as many times as you need to achieve a pass mark of at least 80%.
Timer
To meet the requirements of Licensing Boards this course unit has a timer (see the top of the page) to indicate the amount of time you have spent progressing through the unit. You need to have spent at least 90 minutes working through the materials before you can access the quiz.
Please note the following requirements:
This website automatically saves the time you have spent on this page about every 3 minutes. This means that you need to be on this page for at least 3 minutes for any time to be saved. The timer stops if you log out.
Disclaimer: Please read the Disclaimer at the bottom of this page.
Copyright © Educom Pty Ltd: All content on the acemsk.com website, including text, graphics, videos, and downloadable files, is the property of Educom Continuing Education, a division of Educom Pty Ltd, and is protected by copyright and other intellectual property laws under international conventions. Unauthorized use or duplication of this material without express written permission from Educom Pty Ltd is strictly prohibited.
Content Links
The following buttons can be used to navigate the content in this unit.
Diagnostic Features
Temporomandibular Joint Pain and Dysfunction
Introduction
Temporomandibular Joint Disorders
Temporomandibular joint disorders are commonly seen in clinical practice. They are reported to be more common in women and have a peak age incidence of 20–40 years. Clinical presentations of temporomandibular joint disorders are characterized by acute or chronic pain and may include the following:
- Temporomandibular joint dysfunction
- Facial pain
- Ear pain, a feeling of ear fullness, and tinnitus
- Neck pain
- Orbital pain
- Dizziness
Temporomandibular Joint Dysfunction
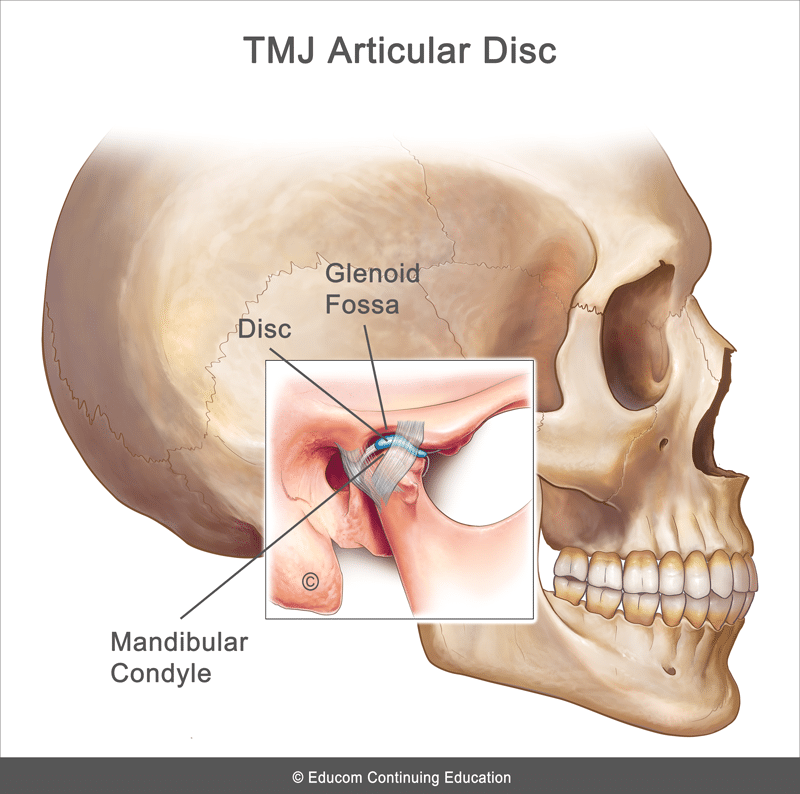
Temporomandibular joint dysfunction is characterized by pain arising from an abnormal relationship between the temporomandibular joint (TMJ) articular disc and the adjacent articular surfaces, as well as the surrounding myofascial structures. The TMJ is an extremely important articulation necessary for mastication, swallowing, facial expression, and communication. This joint is classified as a ginglymoarthrodial joint allowing essentially a hinge-like movement (rotation) combined with a gliding motion (translation). On opening the mouth, the movement begins with rotation of the mandibular condyle in the glenoid fossa, followed by a forward translation of the condyles. The TMJ involves articulation between the mandibular condyle and the glenoid fossa of the temporal bone. These two osseous structures are separated by a fibrocartilagenous disc. The TMJ is strengthened by its joint capsule and several ligaments (the sphenomandibular, stylomandibular, pterygomandibular, malleolomandibular and collateral ligaments).
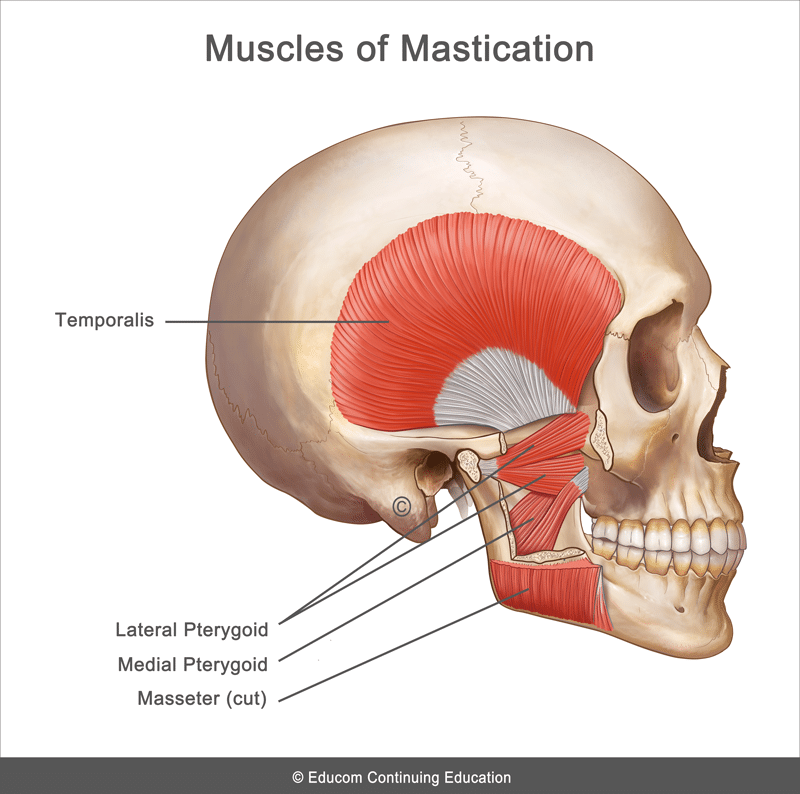
The muscles involved in the opening and closing of the mouth are the primary muscles of mastication, including the masseter, temporalis, and medial pterygoid muscles which elevate the mandible to close the mouth, and the lateral pterygoid muscle which assists in opening the mouth by guiding forward movement of the jaw. Innervation of the TMJ and its associated muscles involves branches of the third division of the trigeminal nerve.
The etiology of TMJ dysfunction is thought to be multifactorial including anatomical, pathophysiological, and psychosocial factors. Musculoskeletal dysfunction is the most common contributing factor to TMJ dysfunction. This could be due to the following:
- Joint trauma
- Muscle imbalance
- Poor head and neck posture
- Myofascial pain syndromes
- Internal joint derangement
- Degenerative joint disease
- Chronic bruxism (clenching or grinding the teeth)
- Dental malocclusion
- A physical manifestation of a psychological disorder (e.g., depression, anxiety, or post-traumatic stress disorder)
Differential Diagnosis of Orofacial Pain
Patients presenting with orofacial pain may be suffering from several conditions. The differential diagnosis includes the following:
- TMJ dysfunction
- Dental caries, abscess, or malocclusion
- Otitis media and otitis externa
- Upper cervical facet joint dysfunction
- Mastoiditis
- Migraine headache
- Cluster headache
- Tension-type headache
- Trigeminal neuralagia
- Post-herpetic neuralgia
- Giant cell arteritis (Temporal arteritis)
- Parotitis
- Mandibular fracture or dislocation
- Sinusitis
- Cancer of the jaw, head, or neck
History
- Preauricular pain that is usually described as deep and aching with sharp exacerbations on jaw movement
- Pain that may refer to the head and neck
- Pain that is aggravated by chewing, yawning, or talking for extended periods
- Joint clicking, popping, or snapping on jaw movement
- Limited jaw opening
- May have jaw-locking
- Headache
- May have associated otological symptoms (e.g., tinnitus, vertigo, earache, or hearing loss)
Physical Examination
- Abnormal mandibular movement
- Decreased TMJ range of motion (inability to fully open the mouth, typically 25 mm or less)
- Local tenderness over the joint and/or in the muscles of mastication
- Palpation may reveal a clicking or popping sensation with jaw movement
- Palpation may reveal grinding or crepitus with jaw movement
- Muscle tension or spasm
- Pain on jaw clenching due to dynamic loading
- May have evidence of tooth wear or malocclusion
- May have abnormal cervical posture
Diagnostic Imaging
The diagnosis of TMJ dysfunction is usually clinical. Plain radiography can help to rule out degenerative joint disease, fractures, dislocations, and bone pathology. Magnetic resonance imaging (MRI) is considered the gold standard for the investigation of TMJ disorders as it is able to assess soft tissue structures, articular disc displacement, and the presence of joint effusion.
Red Flags
The following are examples of red flags for patients presenting with orofacial pain:
- A history of significant injury
- Severe pain
- Unrelenting pain
- Nocturnal pain
- Unexplained weight loss
- Fever
- Deformity
- Trismus
- Significant swelling
- Unilateral hearing loss or a new onset of tinnitus
- Vestibular dysfunction
- Significant loss of range of motion
- Severe tenderness on palpation or severe pain with any examination procedure
If any red flags are identified during history taking and clinical examination, referral for urgent medical evaluation and further investigation is warranted.
TMJ Palpation
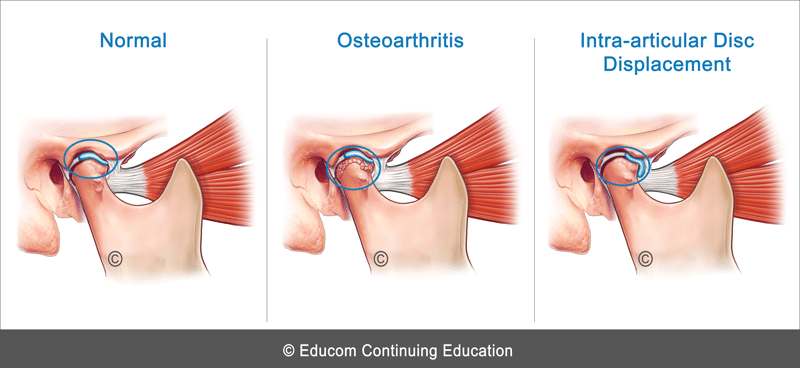
When palpating the TMJ (e.g., by placing fingers in the patient’s ears while they open and close their mouth), if a crackling or grating sound or sensation is present, this suggests osteoarthritis. If a clicking sensation is present, this could indicate displacement of the intra-articular disc.
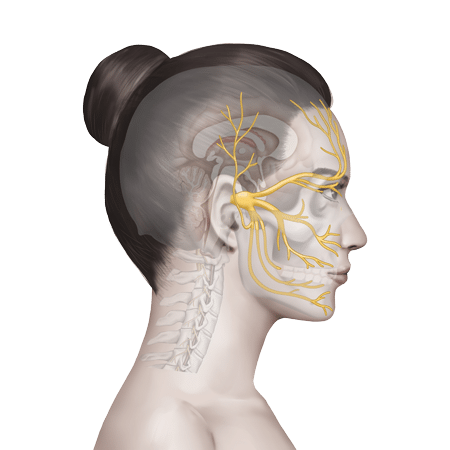
Innervation of the TMJ and Associated Muscles
Since innervation of the TMJ and its associated muscles involves branches of the third division of the trigeminal nerve, pain from mandibular pathology or the mandibular teeth can be referred to the preauricular area and misinterpreted as arising from TMJ dysfunction. On the other hand, pain arising from the TMJ may be perceived by the patient as an earache.
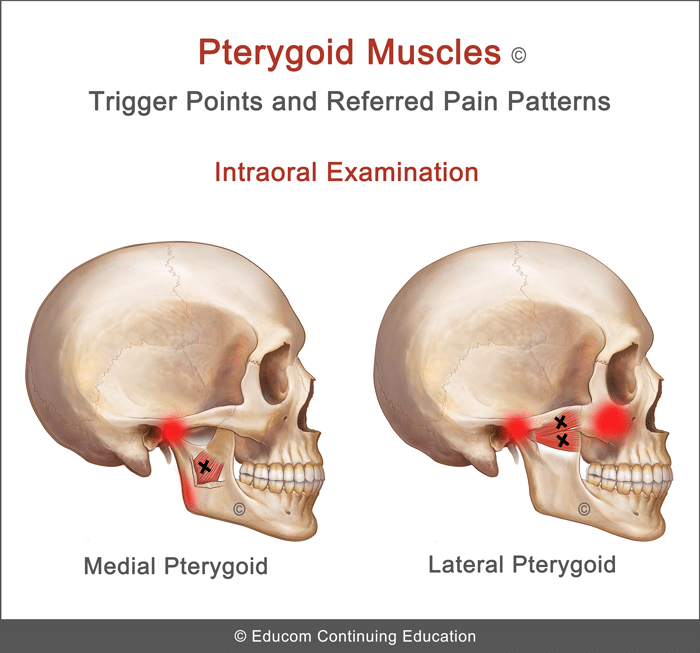
Myofascial Pain Syndrome Presenting as TMJ Pain
In patients presenting with TMJ pain, a complete clinical examination should include an evaluation for the presence of myofascial trigger points as either the primary cause of the pain or as a concomitant condition. The primary muscles to evaluate include the following:
- Medial Pterygoid: Pain primarily in the region of TMJ
- Lateral Pterygoid: Pain primarily in the region of TMJ and maxillary area sometimes resembling as “sinus pain”
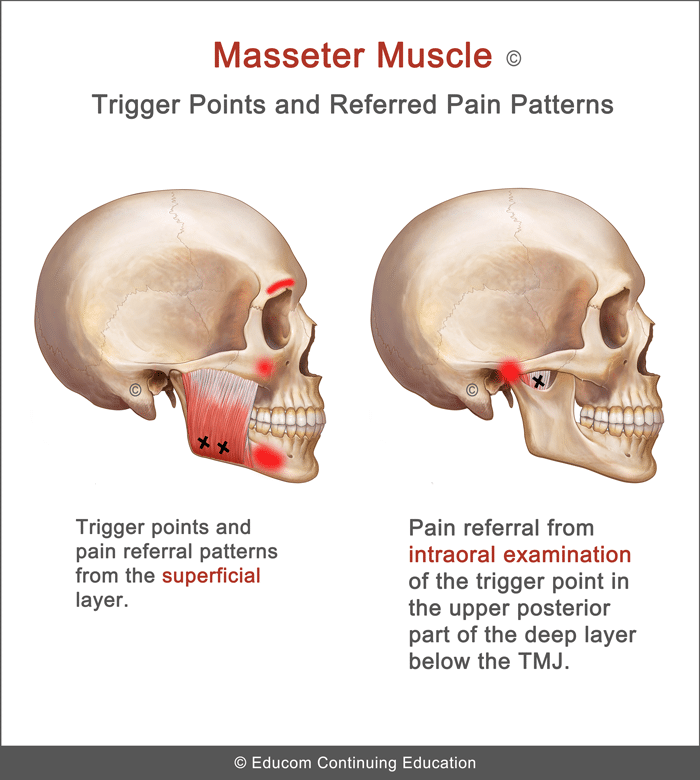
- Masseter – Superficial Layer: Pain primarily in the lowewr jaw and zygomatic arch
- Masseter – Deep Layer: Pain primarily in the TMJ (trigger point palpated intraorally)
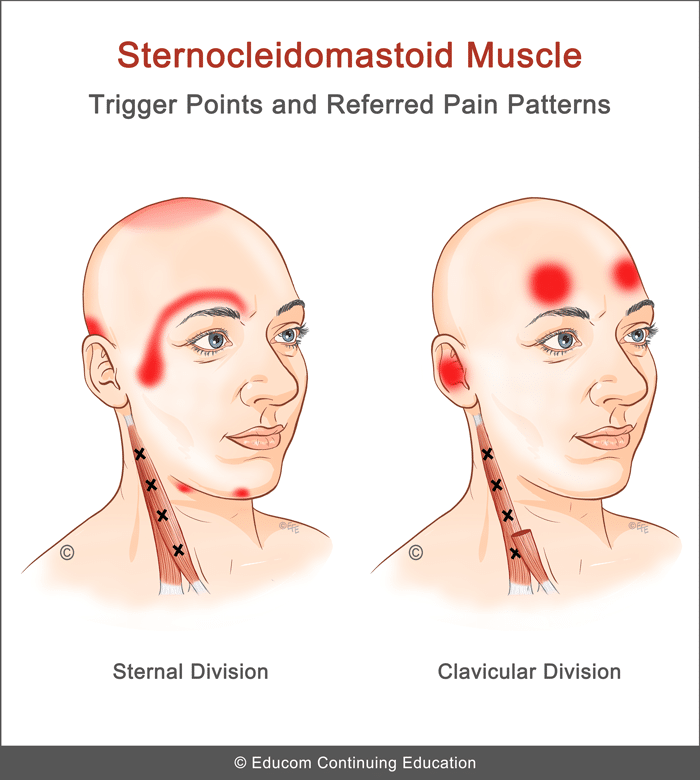
- Sternocleidomastoid – Clavicular Division: Pain primarily in the forehead (may refer to both sides), pain deep in the “ear” with/without feeling of lightheadedness and imbalance
- Sternocleidomastoid – Sternal Division: Pain primarily in the temporal region and deep behind the eye
Management
The suggested conservative therapy, home advice, and clinical tips in this section are based on published materials and the clinical experience of the authors of this course. This should not be interpreted as a prescriptive guide to the treatment of this or any other condition. The use of this content is subject to the “Disclaimer” found at the bottom of this web page.

Acute Phase
- Evaluation and Correction of Joint Dysfunction (if present) – If indicated, any management techniques that are applied should minimize excessive loading. We recommend using a handheld instrument-assisted procedure.
- Low Level Laser Therapy – Some patients benefit from the application of low level laser therapy over the involved TMJ to assist with pain reduction and healing.
- Myofascial Release – If any myofascial pain syndrome is present, treat the trigger points using myofascial release, particularly in the head and neck regions.
- Acupuncture – Some patients benefit from acupuncture treatment.
- Ice – Application of ice over the involved TMJ. The ice pack may be applied for 5 to 10 minutes as often as every hour.
Subacute and Rehabilitation Phase
- Correction of Joint Dysfunction (if present)
- Low Level Laser Therapy
- Acupuncture
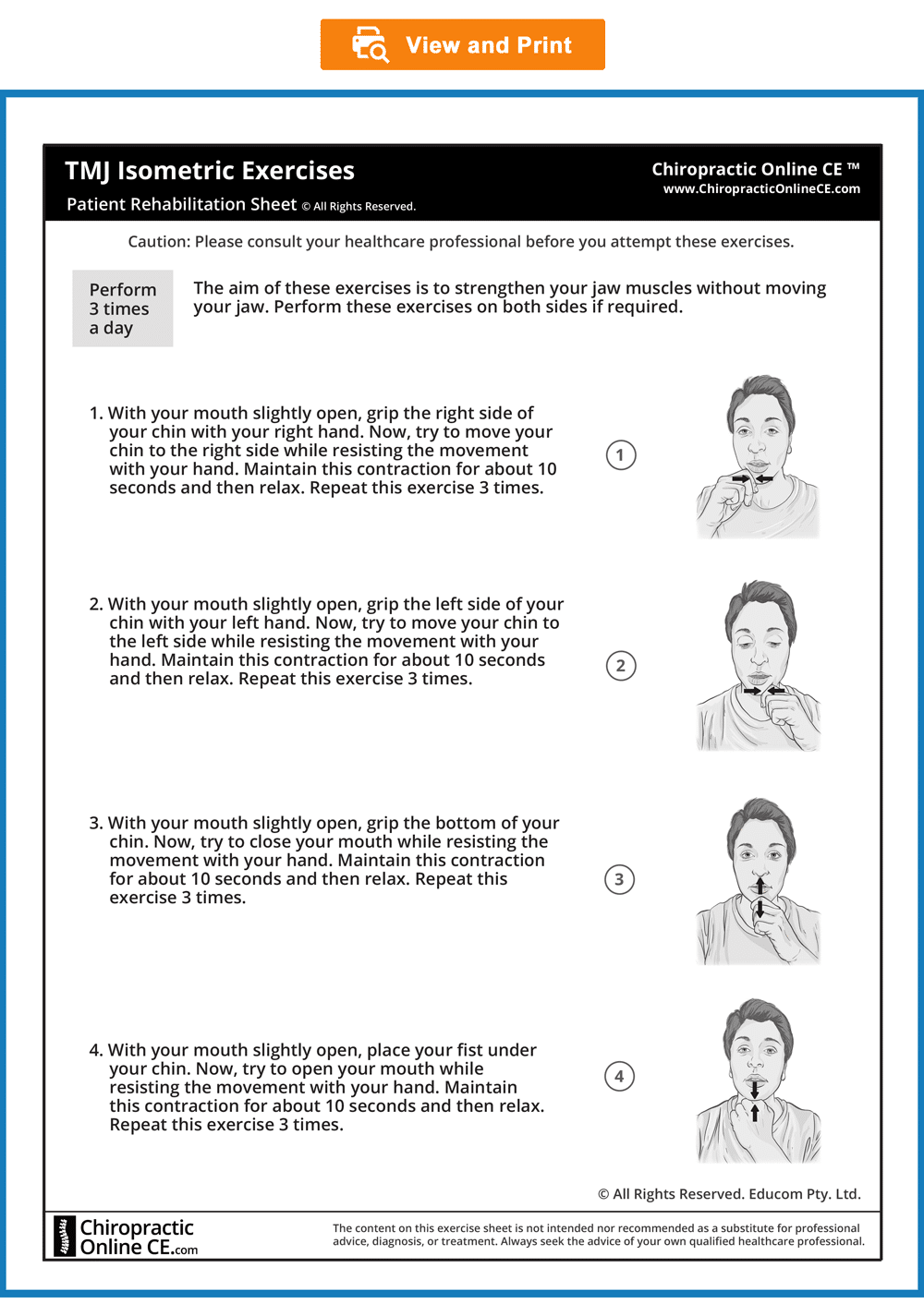
- TMJ Isometric Exercises
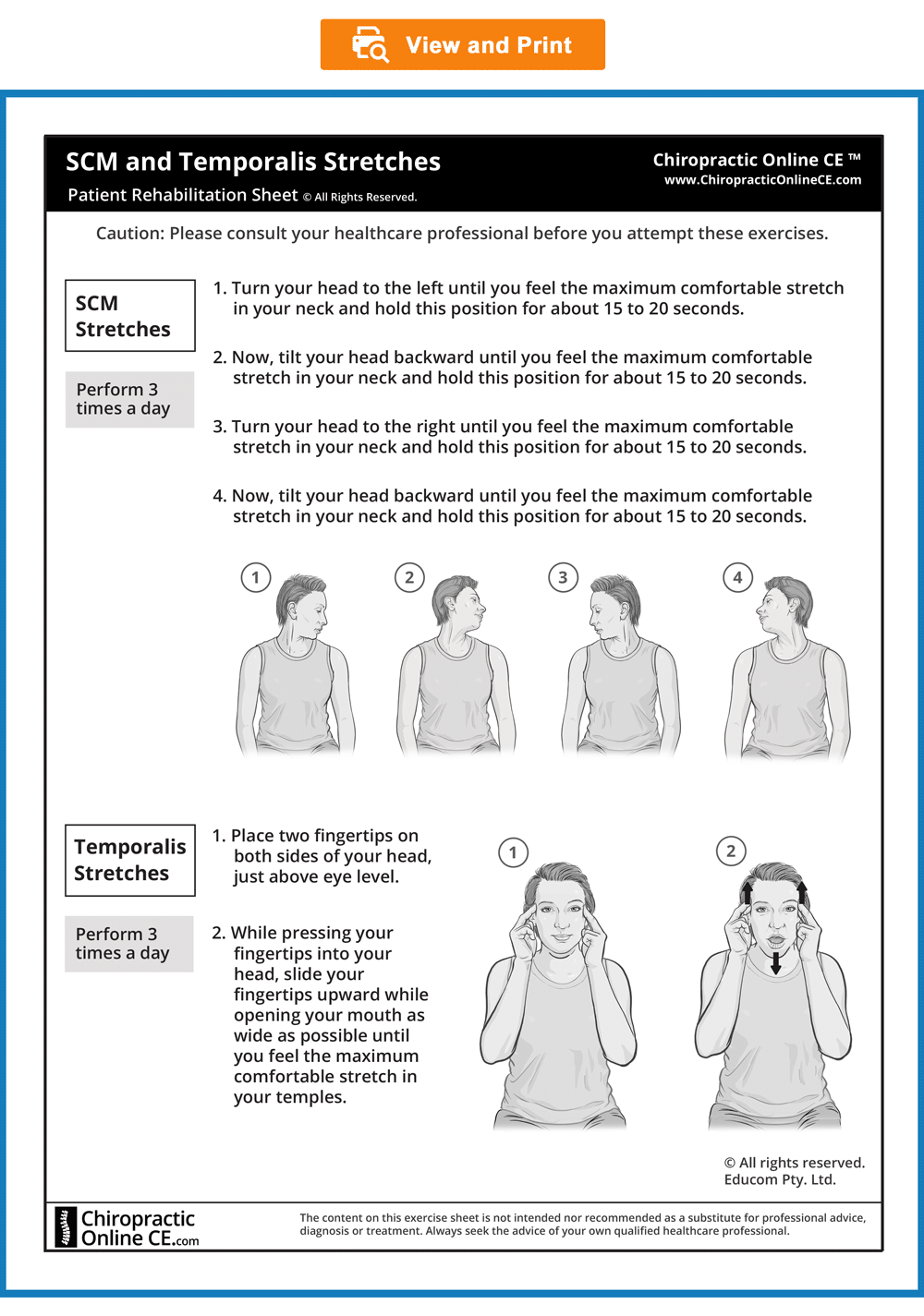
- SCM and Temporalis Stretches
- Ice – Application of ice if the pain returns.
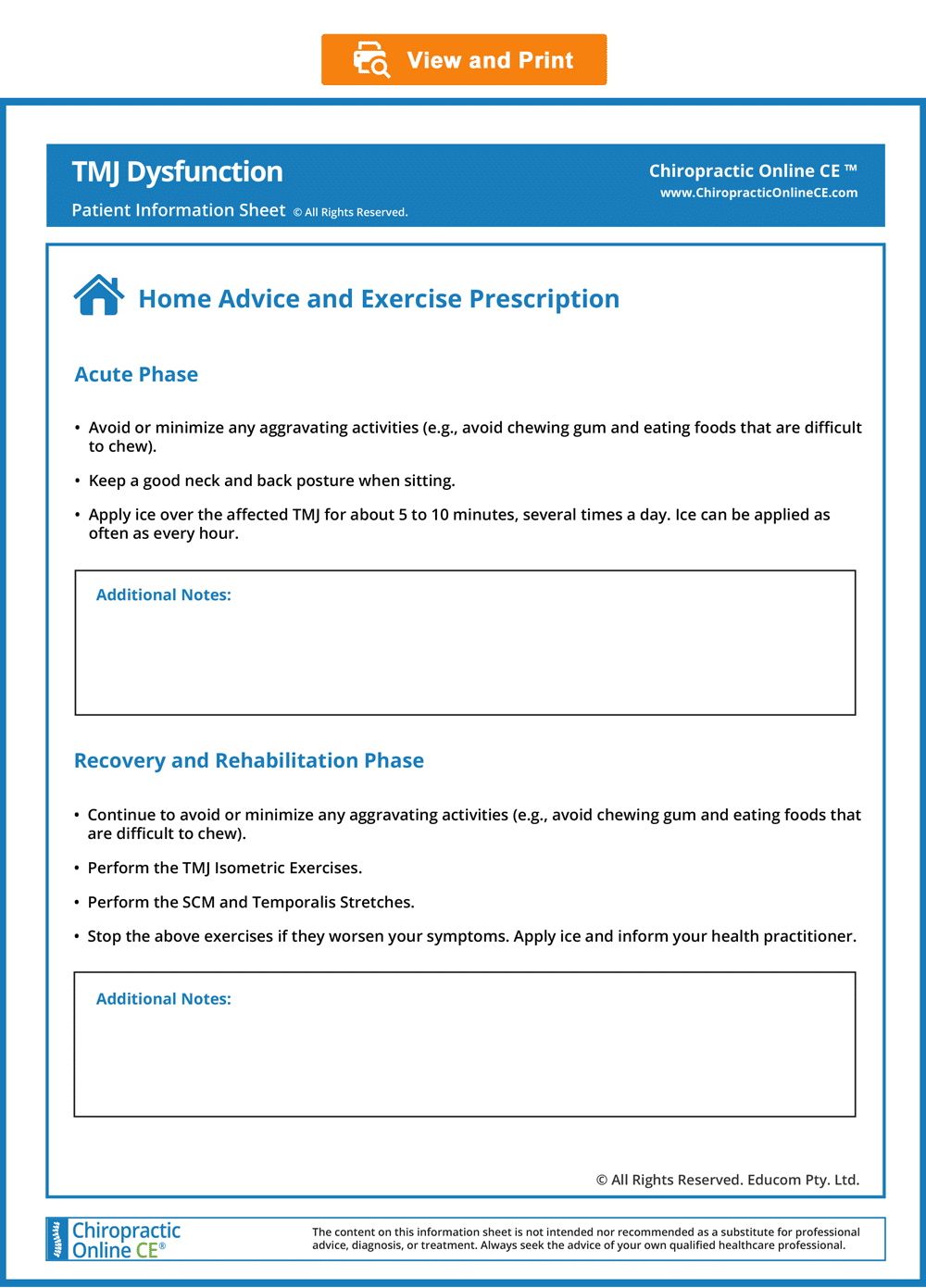
Acute Phase
- Avoid or minimize any aggravating activities (e.g., avoid eating foods that are difficult to chew, including chewing gum).
- Keep a good neck and back posture when sitting.
- Apply ice over the affected TMJ for about 5 to 10 minutes, several times a day. Ice can be applied as often as every hour.
Subacute and Rehabilitation Phase
- Continue to avoid or minimize any aggravating activities (e.g., avoid eating foods that are difficult to chew, including chewing gum).
- Perform the TMJ Isometric Exercises.
- Perform the SCM and Temporalis Stretches
- Stop these exercises if they worsen your symptoms and report it to your practitioner.
- Apply ice if your TMJ pain returns or is aggravated.
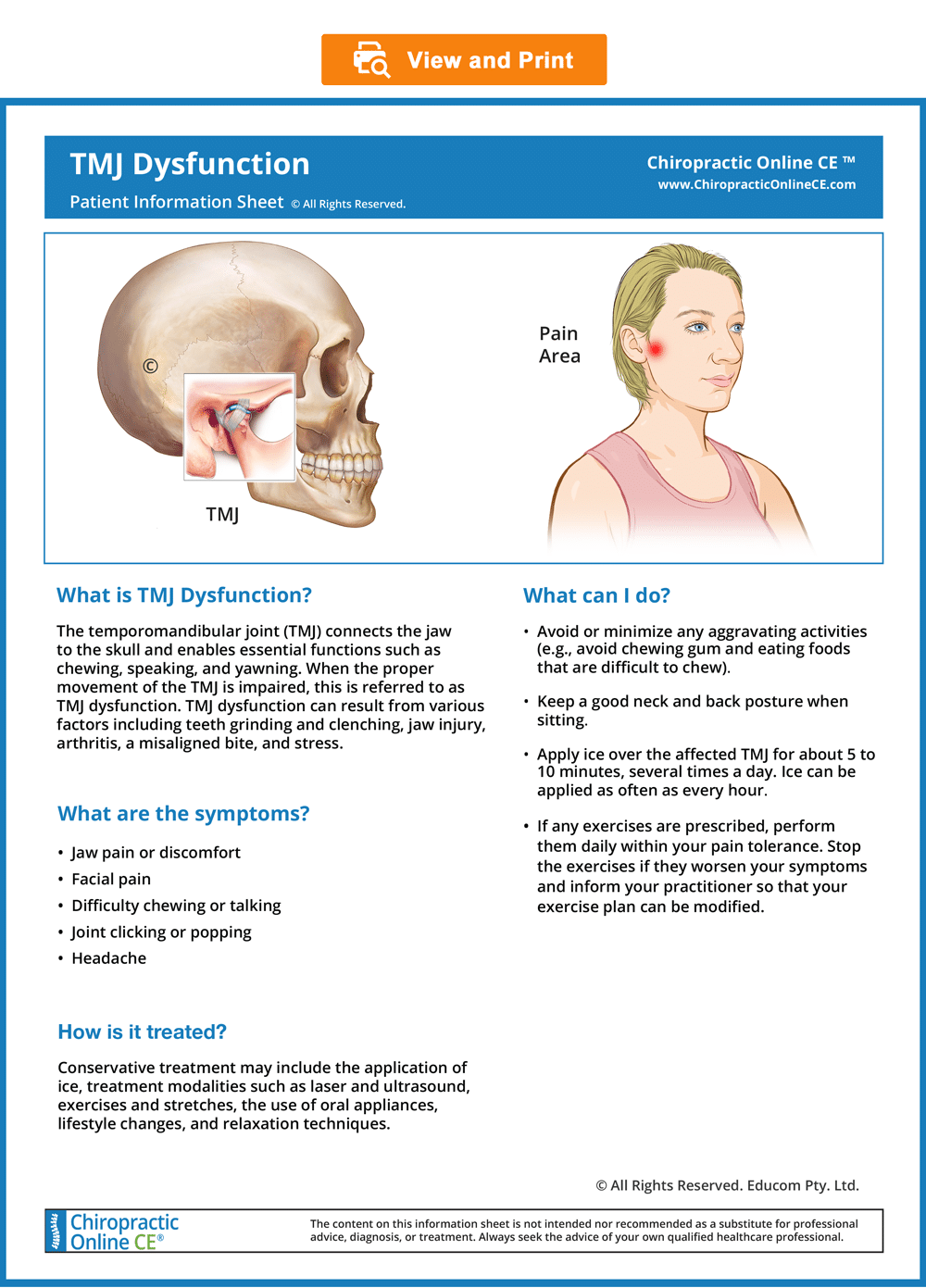
For Patients
Patient Information, Home Advice, and Exercise Prescription Sheets
- You may wish to give your patients the following downloadable and ready-to-use Patient Information, Home Advice and Exercise Prescription sheets. In our experience, patients who are well informed about their condition and the recommended management are more likely to achieve good outcomes, become loyal patients, and recommend their family and friends to seek treatment.
- To view, download, or print these sheets, simply click on the images below.
© Educom Pty. Ltd. All Rights Reserved.
Patient Exercise Sheets
- When appropriate, the patient should gradually begin doing their prescribed exercises at home. Always recommend warm-up activities before commencing specific exercises. Warm-up activities include simple limbering movements or prescribed strength exercises at light loads.
- If stretches are indicated, instruct your patients to perform them after they have completed their strengthening exercises.
- Always recommend warm-up activities before commencing specific exercises. Warm-up activities include simple limbering movements or prescribed strength exercises at light loads.
- Always instruct your patients to use caution when performing their exercises in order to avoid overloading, overstretching, or any undue pain.
- To view, download or print the Patient Exercise Sheet, simply click on the image below.
© Educom Pty. Ltd. All Rights Reserved.
Our Recommended Approach
- Review the Information: Carefully read through the content in each section of the case scenario.
- Consider the Question: To encourage critical thinking, we recommend attempting to answer the “Diagnostic Reasoning Question” on your own before reading our suggested answer. If you prefer, you can hide our suggested answer by clicking the “Suggested Answer” arrow.
- Compare Your Answer: When ready, click the arrow again to reveal our answer and compare it with your own.
Repeat these steps for each section of the case scenario. Please note that the suggested answers are only indicative and not exhaustive. They serve as guidelines and should not be considered complete answers.
Patient’s History
In the sections below, you will find case history information designed to guide you through a systematic approach to performing a focused and relevant case history. This process will help you narrow down the potential causes of the patient’s complaint. As you go through the material, we encourage you to answer the questions provided to test and enhance your diagnostic reasoning skills.
Who is the patient and where is the pain?
When was the onset and what caused the onset?
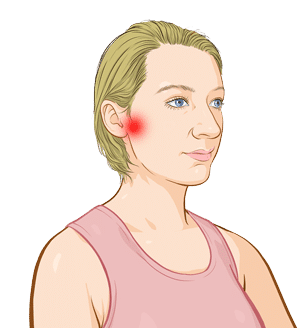
Natalie, a 32-year-old teacher, presents with a two-week history of right-sided facial pain. She identifies the area in front of her right ear as the primary site of discomfort. The pain began within 24 hours after undergoing a prolonged dental procedure to repair a cracked tooth. Natalie has since revisited her dentist, who advised the use of painkillers and suggested that the pain should resolve with time.
|
What differential diagnoses would you consider for Natalie? |
Suggested Answer
Pain in the preauricular region can indicate several conditions, including:
- Temporomandibular joint dysfunction
- Myofascial pain syndromes (e.g., involving the medial and lateral pterygoids, masseter, and sternocleidomastoid muscles)
- Upper cervical facet joint dysfunction
- Dental conditions (e.g., caries, abscess, malocclusion)
- Otitis media and otitis externa
- Trigeminal neuralgia
- Post-herpetic neuralgia
- Giant cell arteritis (temporal arteritis)
- Parotitis
- Mandibular fracture or dislocation
- Cancer of the jaw, head, or neck
|
Based on the patient’s history, how would you differentiate between trigeminal neuralgia and temporomandibular joint (TMJ) dysfunction? |
Suggested Answer
- Trigeminal Neuralgia – Trigeminal neuralgia is characterized by sudden, severe, stabbing, or electric shock-like pain that typically lasts from a few seconds to a few minutes. The pain is usually localized to specific branches of the trigeminal nerve and often affects one side of the face. Light touch, movement, or even routine activities like chewing or speaking can trigger these intense pain episodes.
. - TMJ Dysfunction –Temporomandibular joint (TMJ) dysfunction often presents with pain localized to the temporomandibular joint, which may radiate to the jaw, temples, neck, or surrounding areas. The pain is frequently aggravated by activities such as chewing, clenching the jaw, or other jaw movements. Patients may also experience clicking or popping sounds in the jaw joint, restricted jaw movement, muscle stiffness or tenderness in the jaw or face, and sometimes, headaches.
What are the pain characteristics?
What are the aggravating and relieving factors?
What has been the course of the pain?
Natalie describes the pain as a constant, dull ache with sharp exacerbations triggered by jaw movements, particularly during chewing or yawning. She rates the dull ache at 3 out of 10 in intensity, while the sharp exacerbations reach 9 out of 10. Applying an ice pack directly over the painful area provides temporary relief. Although she initially took painkillers as advised by her dentist, which also offered brief relief, she has since stopped taking them and seeks your assistance to address the underlying issue. The intensity of her pain has remained unchanged since it began.
|
What are the potential causes or underlying conditions that could result in a patient experiencing a constant dull ache in the jaw, with sharp exacerbations triggered by movements such as chewing or yawning? |
Suggested Answer
Her description of pain aggravated by jaw movement strongly suggests involvement of the temporomandibular joint (TMJ), the muscles of mastication, or a dental issue. However, it could also indicate the possibility of an external or middle ear infection.
|
Diagnostic Reasoning Question 2 How does the temporary relief from ice packs and painkillers contribute to our understanding of the underlying condition? |
Suggested Answer
Pain relief from applying an ice pack may suggest an underlying inflammatory process, though it could also reflect an analgesic effect similar to that provided by painkillers.
Are there any associated symptoms?
Upon further questioning, Natalie reveals that the sharp exacerbations of pain are accompanied by a clicking sensation in her right jaw when chewing or yawning. The dull ache in her jaw sometimes radiates to the right side of her head, particularly after a full day of teaching. Additionally, she reports a mild earache on the right side and suspects that her hearing in that ear may be slightly diminished.
|
How does jaw clicking accompanied by pain contribute to the diagnostic process? |
Suggested Answer
An occasional, painless jaw click is common in the general population. However, dysfunction of the temporomandibular joint (TMJ), such as disc displacement or joint degeneration, can lead to sharp pain exacerbations and clicking sensations during jaw movements. Additionally, clicking accompanied by pain when chewing may indicate changes in bite alignment due to dental issues.
|
How does the spread of jaw pain to the side of the head, along with associated symptoms like mild earache and diminished hearing, inform the diagnostic process? |
Suggested Answer
A dull ache in the jaw that spreads to the side of the head, especially after prolonged jaw movement (such as a day of talking), is often consistent with referred pain from TMJ dysfunction. TMJ dysfunction can cause pain to radiate to nearby areas, including the head and neck. However, similar referral patterns can also arise from myofascial pain syndrome, dental issues, or ear infections. Perceived hearing loss might suggest an ear infection, though it has also been reported in cases of TMJ dysfunction.
Is there a past history that is relevant to the current complaint?
Natalie has no past history of jaw pain.
|
How does the absence of a previous history of jaw pain inform the diagnostic process? |
Suggested Answer
Her lack of a previous history of jaw pain suggests that the current issue may be acute or the result of a recent event rather than a chronic or recurring condition.
Are there any “red flags”?
The following questions are asked to identify any “red flags” that could suggest serious pathology. Even if the patient has previously mentioned related information during the case history, it is recommended to revisit these questions to ensure a comprehensive evaluation.
- Do your symptoms disappear even for a short time? “Yes. I am not aware of the pain when I first wake up in the morning.”
- Does the pain wake you up at night? “No.”
- Are you experiencing any dizziness or loss of balance? “No.”
- Have you recently had any fever, chills, or night sweats? “No.”
- Have you recently had an infection or other illness? “No.”
- Have you had any unexplained weight loss recently? “No.”
- Do you have a history of cancer, inflammatory arthritis, or fracture arising from minor trauma? “No.”
|
Do any of the patient’s answers raise a red flag? |
Suggested Answer
None of the patient’s responses raise a red flag.
What is the list of possible causes for the patient’s complaint?
|
Based on the available history, how would you prioritize the list of differential diagnoses? |
Suggested Answer
- Temporomandibular joint dysfunction
- Myofascial pain syndromes (e.g., involving the medial and lateral pterygoids, masseter, and sternocleidomastoid muscles
- Dental malocclusion
- Otitis media and otitis externa
- Upper cervical facet joint dysfunction
Reflection Point
Please pause and consider whether the key elements of a thorough and relevant patient history have been addressed. Are there any additional questions you would have asked? If so, what are they, and why would they be important?
Before reviewing the physical examination findings below, take a moment to reflect on which physical examination procedures you would perform to accurately assess this patient.
Performing Physical Examination
In the sections below, you will find physical examination findings for this patient. The material outlines a systematic approach to conducting a focused and relevant physical examination aimed at narrowing down the potential causes of the patient’s complaint. As you review the material, we encourage you to answer the questions provided to test and enhance your clinical reasoning and diagnostic skills. Additionally, consider whether all essential elements of the physical examination have been thoroughly addressed.
Vital Signs
Natalie’s vital signs are within normal limits.
|
What do normal vital signs mean? |
Suggested Answer
Normal vital signs typically indicate that there are no immediate life-threatening conditions. Normal temperature, in particular, indicates the absence of acute infection.
Inspection
Inspection of the right preauricular area reveals no signs of swelling, redness, or deformity. An otoscopic examination of the right ear is unremarkable, with no abnormalities detected. Additionally, her head and neck posture appear normal upon inspection.
|
How does the lack of visible swelling, redness, or deformity in the preauricular area guide the diagnostic process? |
Suggested Answer
The absence of swelling, redness, or deformity in the preauricular area helps to rule out local inflammation, infection, or bone pathology.
|
How do normal findings from an ear inspection and otoscopic examination impact the diagnostic process? |
Suggested Answer
A normal ear examination helps to rule out conditions such as otitis media and otitis externa.

Range of Motion
The TMJ active movement assessment reveals a reduced jaw opening of only 25 mm, with noticeable deviation to the right, accompanied by pain in the right TMJ. Lateral jaw movement is also limited, particularly to the left, which similarly provokes pain in the right TMJ. In contrast, both active and passive cervical range of motion assessments are found to be normal.
|
What do the findings from the TMJ active movement assessment suggest? |
Suggested Answer
The findings suggest TMJ dysfunction, potentially caused by:
- Hypertonicity or imbalance in the muscles of mastication
- Displacement of the TMJ meniscus, interfering with the normal forward movement of the mandibular condyle
- TMJ pathology, such as arthritis or local osseous issues
The normal cervical range of motion assessment helps to rule out cervical spine involvement.
If you’d like to see how the TMJ active movement assessment is performed, please watch the video below.
The resisted jaw movement assessment reveals an increase in the patient’s pain during resisted jaw closure and when resisting jaw deviation to the left.
|
How do the findings from the resisted jaw movement assessment contribute to the diagnostic process? |
Suggested Answer
TThese findings provide further evidence of TMJ dysfunction, potentially caused by an intra-articular disorder or involvement of the muscles of mastication.
If you would like to see how the resisted jaw movement assessment is performed, please watch the video below.
Palpation
Palpation of the right TMJ reveals tenderness, with jaw opening and closing producing a clicking sensation accompanied by pain. Additionally, the right mandibular condyle is observed to have inadequate forward sliding. Muscle palpation indicates tenderness in the right medial and lateral pterygoid, temporalis, and masseter muscles. No nodules or pain referral to the TMJ are detected on palpation of the masseter or SCM muscles. The right ear, mastoid process, and parotid gland are non-tender on palpation. A functional examination of the cervical vertebral motion segments is normal.
|
How do the palpation findings of tenderness in the right TMJ, pain with a clicking sensation during jaw movement, and insufficient forward sliding of the right mandibular condyle collectively inform the diagnostic process? |
Suggested Answer
The TMJ tenderness, clicking sensation, and inadequate forward movement of the right mandibular condyle strongly support a diagnosis of TMJ dysfunction.
|
How do the palpation findings of tenderness in the right pterygoid, temporalis, and masseter muscles, combined with the absence of nodules and pain referral in the masseter and SCM, contribute to the diagnostic process? |
Suggested Answer
The tenderness on palpation of the masticatory muscles supports the presence of TMJ dysfunction. The absence of nodules and pain referral to the TMJ upon palpation of the masseter and SCM helps to rule out myofascial pain syndrome involving these muscles.
If you would like to see how a palpation examination of the TMJ and the muscles of mastication is performed, please watch the video below.
Neurological Examination
A cranial nerve examination reveals no abnormalities, with no sensory disturbances detected in the trigeminal nerve distribution.
|
How does the absence of sensory disturbances in the trigeminal nerve distribution enhance your understanding of the patient’s jaw pain? |
Suggested Answer
The absence of sensory disturbances within the trigeminal nerve distribution indicates that the trigeminal nerve is likely not involved, further supporting TMJ dysfunction as the most probable diagnosis.
If you would like to see how a cranial nerve examination is performed, please watch the video below.
Reflection Point
Considering the patient’s history and examination findings thus far, please take a moment to reflect on which special tests would be most appropriate to further evaluate this patient.
Special Tests
The Weber and Rinne tests are performed and are found to be normal.
|
What do normal Weber and Rinne test results indicate in this patient? |
Suggested Answer
Normal findings for the Weber and Rinne tests suggest no significant conductive or sensorineural hearing loss, which helps to rule out ear pathology as a contributing factor to the patient’s symptoms. This further directs the focus towards TMJ dysfunction or other non-auditory causes of jaw pain and associated symptoms.
To see how these tests are performed, please watch the videos below.
The Axial Cervical Compression test yields a negative result, with no localized upper neck pain or referral to the preauricular region.
|
What does a negative result for this test indicate in a patient with jaw pain? |
Suggested Answer
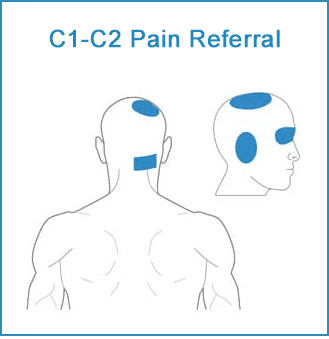
The Axial Cervical Compression test is primarily used to assess for nerve root involvement in the cervical spine. Although it’s not directly related to evaluating jaw pain, it can offer valuable insights in cases where cervical spine pathology might contribute to or mimic jaw pain. Involvement of the cervical facet joints, particularly the C1-C2 facet joints, can lead to localized neck pain or referred pain to the skull. As shown below, specifically, these joints may cause pain referral to the preauricular, occipital, and orbital regions, as well as the vertex. The negative result of this patient’s Axial Cervical Compression test suggests that the upper cervical facet joints are not involved.
Please watch the video below to see how the Axial Cervical Compression test is performed.
Reflection Point
Please stop and take a moment to consider whether all the elements of an adequate and relevant physical examination have been completed for this patient. Are there any additional procedures you would have performed and, if so, why?
Diagnosis
Based on the available information, what is the most likely diagnosis?
View Suggested Answer
Right TMJ dysfunction.
References and Suggested Further Readings:
Pavia S. et al. Chiropractic Treatment of Temporomandibular Dysfunction: A Retrospective Case Series. J Chiropr Med. 2015 Dec;14(4):279-84.
Lomas J. et al. Temporomandibular dysfunction. AJGP. Volume 47, Issue 4, April 2018.
Travell J. Temporomandibular joint pain referred from muscles of the head and neck. J Pros Dent. 1960;10:745.
Shanavas M. et al. Transcutaneous electrical nerve stimulation therapy: An adjuvant pain controlling modality in TMD patients – A clinical study. Dent Res J (Isfahan). 2014 Nov;11(6):676-9.
Ba S. et al. Ultrasound is Effective to Treat Temporomandibular Joint Disorder. J Pain Res. 2021 Jun 10;14:1667-1673.
Disclaimer: The Chiropractic Online CE™ website (including text, graphics, downloadable resources, and videos) is intended to provide general health information for educational purposes only. This information is not a substitute for personal consultation with a qualified healthcare professional. Always seek the advice of a healthcare professional for any questions regarding your condition, symptoms, and appropriate treatments..
Copyright © Educom Pty Ltd: All content on the chiropracticonlinece.com website, including text, graphics, videos, and downloadable files, is the property of Educom Continuing Education, a division of Educom Pty Ltd, and is protected by copyright and other intellectual property laws under international conventions. Unauthorized use or duplication of this material without express written permission from Educom Pty Ltd is strictly prohibited.
This CE unit has a timer (see the top of the page).
You need to have spent at least 90 minutes working through the materials before you can access the quiz.
Quiz: This concludes the learning material for this unit. You may review the material or take the multiple-choice quiz for this unit now or at a later time. You can attempt the quiz as many times as you need to achieve a pass mark of at least 80%.
To take the quiz click the button below.