
Free Sample – Proximal Tibiofibular Dysfunction: Diagnosis and Management (Preview)
Practice Resources
For quick access, the links to the downloadable Practice Resource PDF files for this condition are available below.
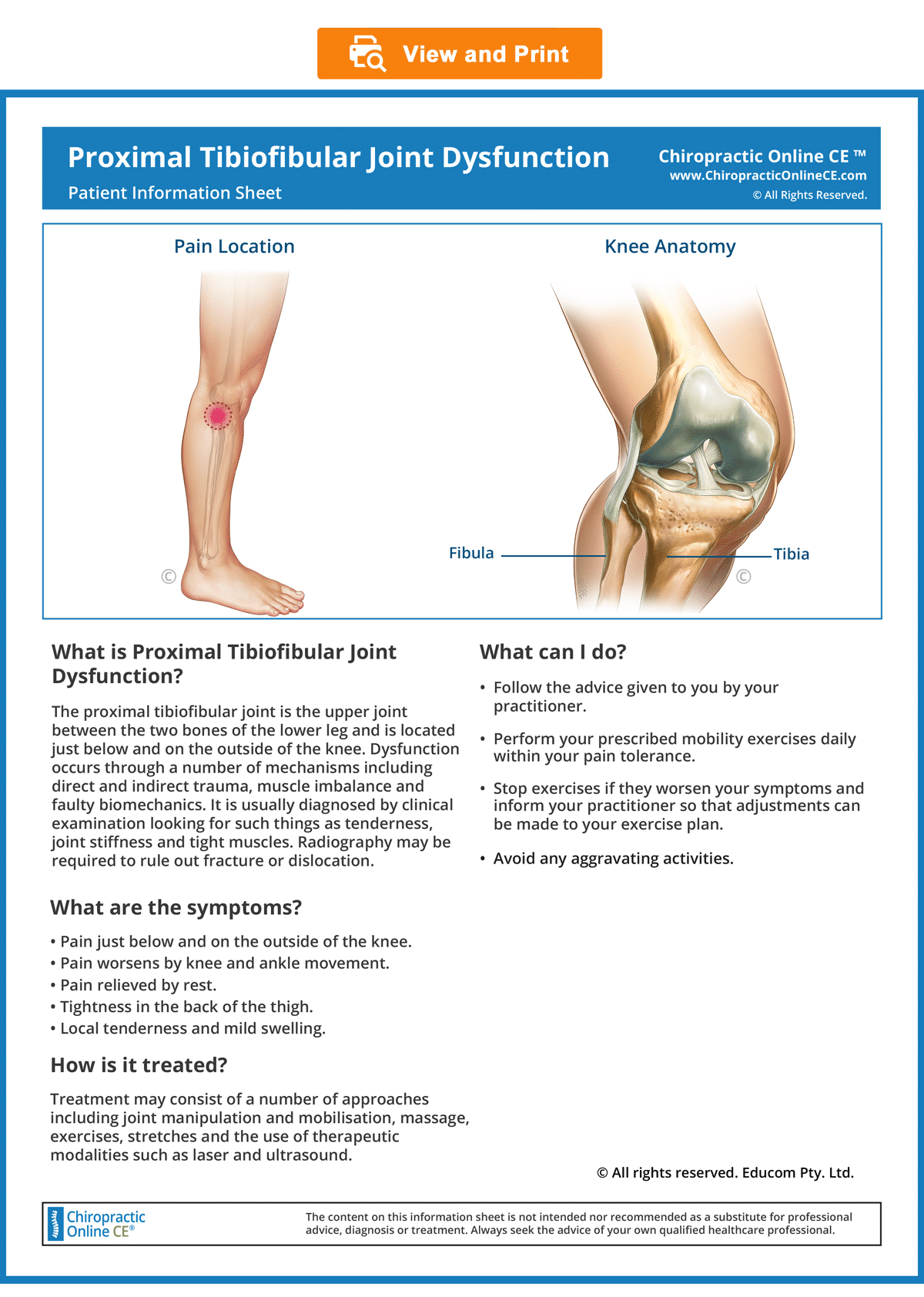
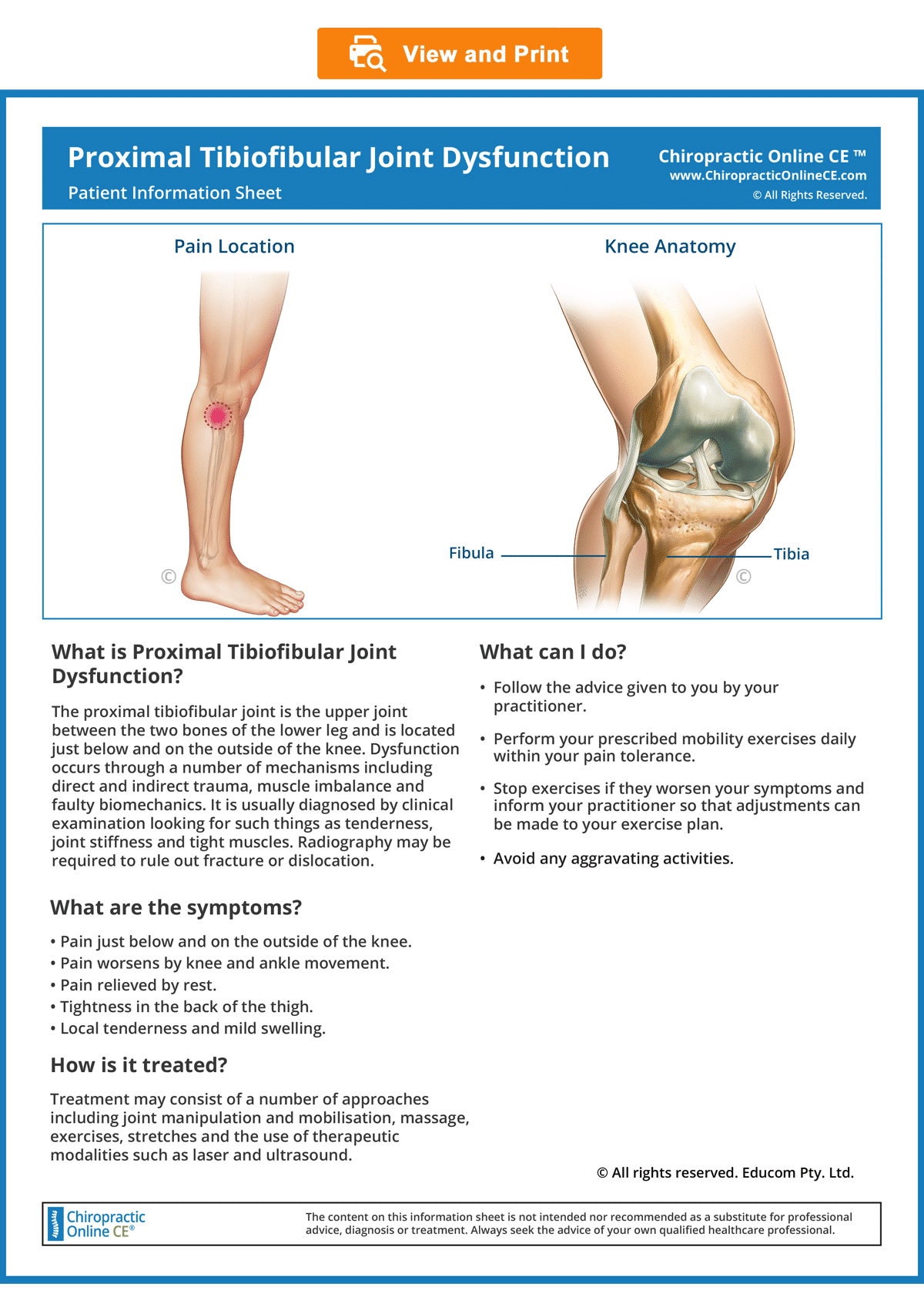
Patient Information Sheet
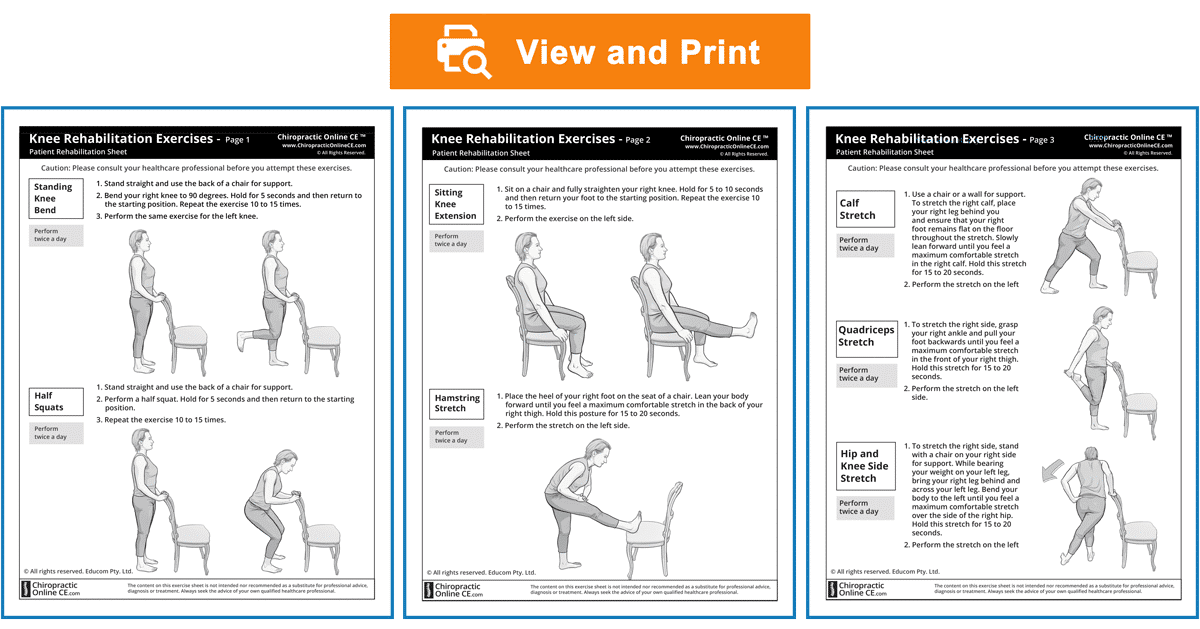
Knee Rehabilitation Exercise Sheets
Please note:
The following sample material is from the course “Clinical Excellence in the Diagnosis and Treatment of Musculoskeletal Disorders- Volume 1”.
Disclaimer: Please read the Disclaimer at the bottom of this page.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.

Part 1: Diagnostic Features and Management
Classic Presentation
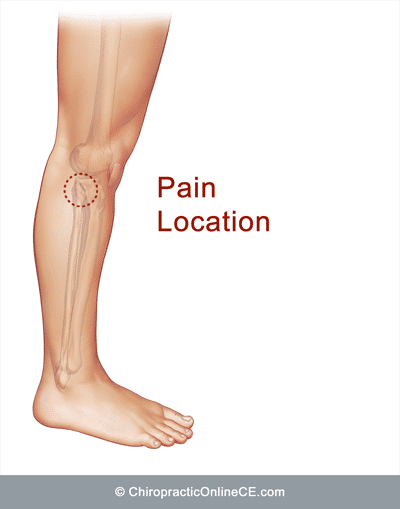
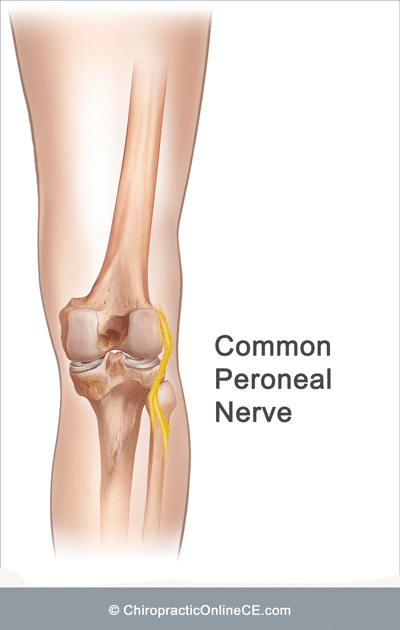
• Lateral knee pain (which may radiate distally if the common peroneal nerve is also involved)
• Pain aggravation with knee and ankle movement (particularly ankle dorsiflexion)
• Pain relieved by rest
 .
. 
Cause
• Direct impact injury to the lateral knee
• Indirect injury caused by excessive loading of the ankle or knee
• Ligamentous instability
Clinical Evaluation
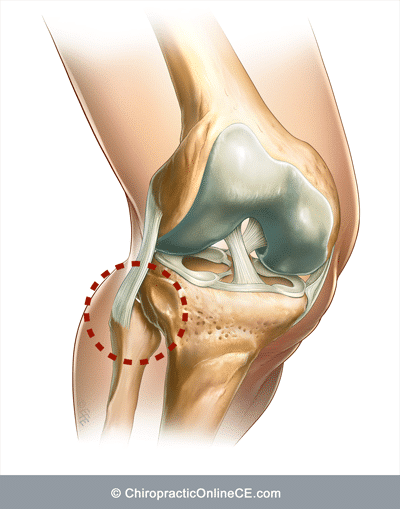
• Pain on palpation of the proximal tibiofibular joint or fibular head
• Local swelling in the region of the proximal tibiofibular joint
• Reduced fibular head motion (proximal tibiofibular joint dysfunction)
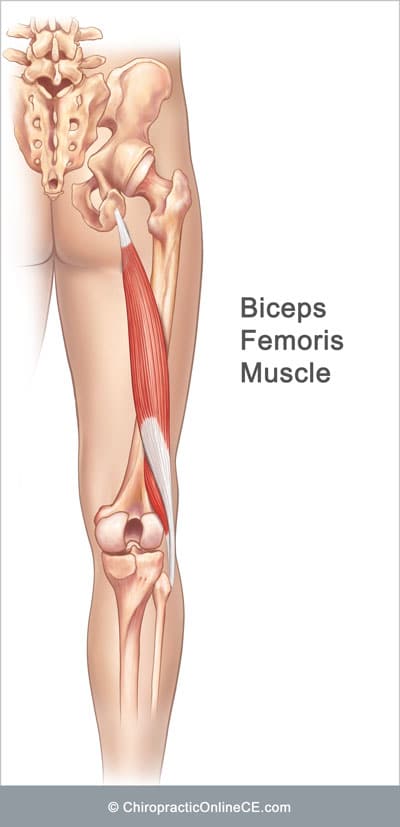
• Tightness in the hamstring muscles (particularly in the biceps femoris)
• Reduced knee extension caused by tightness in the hamstring muscles
Imaging
• Referral for plain film radiography if dislocation, fracture or bone pathology is suspected.
Red Flags
Examples of red flags in patients presenting with knee pain:
• Severe pain
• Inability to bear weight
• Moderate to severe swelling
• Extensive bruising
• Deformity
• Severe tenderness on palpation or severe pain with any examination procedure
If any red flags are identified during history taking and clinical examination, referral for urgent medical evaluation and further investigation is warranted.
When the Patient’s Evaluation Reveals Red Flags
When “red flags” are identified, serious conditions including infection, fracture, dislocation or tumors need to be ruled out before any treatment can commence.
• Refer for medical evaluation and further investigation.
• See a sample referral letter below. You are encouraged to include more information in the letter if required (e.g. the suspected diagnosis or a list of differentials for the patient).
[Date]
[Medical Practitioner’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
Thank you for seeing [Patient’s Name] who presented at my clinic today with the following clinical history and examination findings: [specify – below are some examples]
• A history of severe trauma
• Knee deformity following trauma
• Unrelenting and/or nocturnal pain
• Extensive bruising in the right/left knee
• Moderate to severe swelling, warmth and restricted movement at the right/left knee
• An inability to bear weight on the right/left leg
• Knee pain and fever
I have discussed my concerns regarding the above findings with the patient and have recommended that they see you for a medical evaluation immediately.
I would be grateful if, with [Patient’s Name]’s consent, you would inform me of the results of your assessment and investigation.
Thank you for your evaluation please do not hesitate to contact me if you require further information.
Yours sincerely,
[Your Name]
[Your Qualifications]
Patient Management
If no red flags are identified or further investigations do not reveal any contraindications to treatment, management of the condition may begin.
Purpose
The overall purpose of treatment and rehabilitation is to return the patient to preinjury status as soon as possible. As such, the patient’s management plan needs to include the required elements of an effective therapeutic and rehabilitation program.
Goals
• To eliminate pain
• To restore function
• To rehabilitate the region and provide advice to prevent reinjury

For a faster patient recovery, we advocate a management approach that includes all of the following components:
• A gentle correction of joint dysfunction
• The inclusion of soft tissue therapy
• The provision of support and home advice
• The inclusion of rehabilitation exercises
Please Note: The management approach outlined below is based on published materials (see the References section at the end of this web page) and the clinical experience of the authors of this course. This should not be interpreted as a prescriptive guide to the treatment of this or any other condition. The use of this content is subject to the Disclaimer found at the bottom of this web page.
Treatment and Home Advice
Correction of Joint Dysfunction
• A gentle correction of the dysfunctional tibiofibular joint.
• Evaluation and correction of any dysfunctional joint (if present) along the kinetic chain with emphasis on the foot (particularly the distal tibiofibular joint), ankle, pelvis and spine.
We recommend using an instrument-assisted procedure to avoid or minimize further strain to the joint capsule and ligaments. Others may advocate manual manipulation using a high-velocity short amplitude thrust or mobilization.
When injuries result in tibiofibular joint dysfunction, it is common for irritation of the common peroneal nerve as it passes behind the joint to be present. As such, the manipulative method for treating tibiofibular joint dysfunction should be carefully considered in order to avoid nerve irritation.
Soft Tissue Therapy
Electrotherapy: Some patients benefit from the application of ultrasound phonophoresis and/or low-level laser over the involved soft tissue to assist with pain reduction and soft tissue healing.
Myofascial Release: The application of trigger point therapy or other soft tissue procedures to any of the affected muscles (particularly the biceps femoris muscle).
Support
If required, ask the patient to wear a soft brace to prevent excessive movements that would worsen the injury.
Home Advice
Ask the patient to:
• Avoid any aggravating activities (e.g. prolonged standing or walking, climbing stairs and squatting).
• Apply ice over the affected region for about 10 minutes, several times a day for pain control. Ice can be applied as often as every hour.
Our primary reason for recommending the application of ice at home is to help decrease the patient’s pain which then allows them to tolerate some movement in the location of the injury. This helps the patient to maintain a good range of motion, simulates circulatory perfusion and prevents potential atrophy, all of which help to speed recovery from injury.
We have observed that most patients fail to apply ice immediately following an injury. We encourage patients to always apply ice immediately after any sprain or strain. We explain to them that after an injury, the circulatory disturbance not only causes low blood flow (hypoxia) to the injured area, it also affects the surrounding tissue that was not damaged due to the injury. Hypoxia has the potential to deprive the “non-injured” tissue of adequate oxygen and nutrients, thus damaging those tissues as well. By applying ice immediately after an injury, we are able to reduce the metabolic rate in the “non-injured” tissue so that the tissue can survive better with less blood circulation. This approach helps to limit the total area of tissue damage which, in turn, reduces the overall recovery time. The smaller the area of damaged tissue, the quicker the patient’s recovery.
The patient can apply the ice as often as every hour but each time only for 10 minutes.
Patient Information
Patient Information
Provide information to the patient about the condition to improve their understanding of the condition and enhance compliance (see the downloadable ready-to-use Patient Information Sheet below).
Please note that the bottom right-hand corner of the Patient Information Sheet has been intentionally left blank to allow you to attach your business card.
We encourage our patients to show the information sheets to their family, friends and their medical practitioner, all leading to new patient referrals.
To view, download or print the Patient information sheet, simply click on the image below.
© Educom Pty. Ltd. All Rights Reserved.
Patient Information Sheet
Exercise Prescription
General Principles of Exercise Prescription
• When appropriate, the patient should gradually begin doing exercises at home.
• Always recommend warm-up activities before commencing specific exercises. Warm-up activities include simple limbering movements or prescribed strength exercises at light loads.
• Instruct your patients to perform any strengthening exercises before they perform any stretching exercises.
• Always instruct your patients to use caution when performing their rehab exercises in order to avoid overloading, overstretching or any undue pain.
• Emphasize that they should stop any exercises that cause them concern and seek your advice at the earliest opportunity.
Provide rehabilitation exercise sheets to your patients (see the downloadable ready-to-use Rehabilitation Sheets below).
Download and print out the rehabilitation exercise sheets.
Choose the exercises that you consider to be most appropriate for your patient’s stage of recovery and strike out those that are not required.
We encourage our patients to show their exercise sheets to their family, friends and even their medical practitioner, all leading to new patient referrals.
© Educom Pty. Ltd. All Rights Reserved.
Knee Rehabilitation Exercises
Courtesy Letter to the Patient’s Medical Practitioner
Writing a letter to your patient’s medical practitioner (with the patient’s consent) to advise them that you have commenced treatment for the patient helps to demonstrate your professional knowledge, clinical skills and willingness to collaborate with the medical practitioner in caring for the patient. This approach is effective in improving awareness of the range of treatment modalities you can provide at your practice and could encourage the medical practitioner to refer new patients to your practice.
You will see a sample referral letter below. You are encouraged to include more information in the letter if required (e.g. case history, examination findings and the full management plan).
[Date]
[Doctor’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
I am writing to advise you that [Patient’s Name] has presented at my clinic with [right/left] acute lateral knee pain which I have diagnosed as proximal tibiofibular joint dysfunction. [Patient’s Name] advised me that you are their medical practitioner and has provided consent for me to contact you.
I have commenced a management plan that includes a gentle adjustive procedure to improve knee alignment and function, as well as myofascial release and therapeutic ultrasound to facilitate soft tissue recovery. I have also provided the patient with an information sheet about the condition to increase compliance and rehabilitation exercise sheets to hasten recovery and help prevent re-injury. Copies of these resources are attached to this letter for your reference.
Please do not hesitate to contact me if you require further information or have any suggestions.
Yours sincerely,
[Your Name]
[Your Qualifications]
If the Patient is Not Responding to Treatment
If the patient is not responding to treatment:
• Re-evaluate the patient’s clinical presentation.
• If an alternate disorder that is within your scope of practice is uncovered, manage appropriately. If not, refer the patient for further evaluation.
• See a sample referral letter below. You are encouraged to also include the date of the first presentation, case history and examination findings that led you to your diagnosis).
[Date]
[Medical Practitioner’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
Thank you for seeing [Patient’s Name] who presented at my clinic with [side] lateral knee pain which I diagnosed as proximal tibiofibular joint dysfunction. I implemented a management plan that included a gentle adjustive procedure to improve knee alignment and function, myofascial release and therapeutic ultrasound to facilitate soft tissue recovery, bracing and rehabilitation exercises. The patient’s response has been unsatisfactory to date and therefore I am referring them to you for your evaluation and consideration.
Thank you for evaluating the patient and please do not hesitate to contact me if you require further information.
Yours sincerely,
[Your Name]
[Your Qualifications]
Proximal Tibiofibular Dysfunction
Part 2: Clinical Case Scenario
Please read the following material and watch the videos.
A Problem-Solving Approach to History Taking and Physical Examination
The learning material in this unit is designed to improve your skills in history taking and physical examination. The material includes examples of clinical findings and their analysis using a problem-solving approach. As you read through the material and watch the videos, you are encouraged to identify whether all the required elements of history taking and physical examination have been adequately covered.
Patient’s History
Read the following case scenario to refresh and improve your clinical reasoning when taking the patient’s case history. When taking the patient’s history, the practitioner needs to obtain sufficient information to cover the following essential elements.
Who is the patient and where is the pain?
When was the onset and what caused the onset?
A 26-year-old male presents complaining of sudden onset of right lateral knee pain. He points to the region of the fibular head as the site of pain. He says that he landed awkwardly four days ago during a game of football and immediately felt a sharp pain on the outside of his right knee. The pain became worse later in the evening and into the following day.
Analysis: This is an acute injury arising out of physical activity. Injuries such as joint sprain, ligament tear and muscle strain will need to be considered.
The lateral knee region is a common pain location and can indicate a number of conditions. Those that could result from an acute trauma include:
• Lateral meniscus tear
• Iliotibial band syndrome
• Lateral collateral ligament sprain
• Tendinitis of popliteus or biceps femoris
• Proximal tibiofibular joint dysfunction
• Posterolateral corner injuries
• Proximal fibular fracture
In addition to the above possibilities, some pre-existing conditions affecting the region which may be exacerbated by trauma include:
• Proximal tibiofibular joint osteoarthritis
• Pathological fracture of a tumor of the proximal fibula (e.g., osteochondroma or osteosarcoma)
What are the pain characteristics?
What are the aggravating and relieving factors?
What has been the course of the pain?
He describes the pain as an ache with sharp exacerbations with some activities. He rates the pain intensity as an 8 out of 10 at its worst. He says that the activities that bring on a sharp but only momentary stab of pain include walking downstairs and squatting. He says that he noticed some swelling over the lateral side of the knee the day following the injury which has diminished since. Using ice has provided some temporary relief and he reports that the pain has begun to ease over the last 24 hours.
Analysis: The aching pain, accompanied by sharp exacerbations, also suggests a mechanical cause such as a joint sprain, ligament tear or muscle strain. The description of a sharp pain brought on by activity such as walking downstairs and squatting reinforces the possibility of a mechanical injury.
Swelling localized to the lateral side of the knee may indicate inflammation of a tendon or ligament insertion, of a bursa or of the tibiofibular joint capsule. If it was located directly over the tibiofemoral joint space it could indicate a meniscal cyst which is nearly always associated with meniscal tears. The temporary relief from the application of ice may indicate local inflammation but it could also reflect the analgesic effect of cryotherapy. The recent easing of the pain intensity points to an improvement in the condition and possibly a reduction in inflammation.
Are there any associated symptoms?
He says that since the onset of the knee pain he has noticed a tight discomfort in the back of his right thigh and right posterior pelvis. He has noticed that he is unable to fully straighten his knee, particularly when in a seated position.
Analysis: The description of the posterior thigh and pelvis symptoms may indicate secondary muscle involvement, neural involvement or pain referral from a myofascial pain syndrome, damaged ligaments or tendons.
The inability to fully straighten the knee on the involved side could indicate hypertonicity of the hamstrings, sciatic nerve inflammation or a loose body within the knee although the latter would not be influenced by the position of the hip.
Is there a past history that is relevant to the current complaint?
He recalls similar pain 6 months ago following a collision with another player. He did not seek treatment and the condition resolved within a week.
Analysis: The history of a previous injury to the area of complaint is likely to have predisposed him to the current condition suggesting damage to supporting structures such as ligaments and tendons.
Are there any “red flags”?
The patient is asked the following questions in order to identify any “red flags” that could indicate serious pathology. Even if the patient has already provided information in the case history that relates to these questions, it is recommended that they are readdressed to ensure a thorough exploration.
• Does your pain disappear even for a short time? “Yes. The pain disappears with rest and is also relieved when I apply ice.”
• Does the pain wake you up at night? “No.”
• Do you feel weak in your legs? “No.”
• Have you recently had any fever, chills or night sweats? “No.”
• Have you lost any weight recently? “No.”
• Have you recently had any knee surgery or knee injection? “No.”
• Have you recently had an infection or other illness? “No.”
• Have you recently suffered any knee trauma? “No.”
Analysis: None of the patient’s responses raises a “red flag”.
What is the list of possible causes for the patient’s complaint?
Based on the available history the list of possible causes for the patient’s complaint includes:
• Iliotibial band syndrome
• Lateral collateral ligament sprain
• Tendinitis of popliteus or biceps femoris
• Proximal tibiofibular joint dysfunction
• Posterolateral corner injuries
• Lateral meniscus tear
• Proximal fibular fracture
Reflection Point
Please stop and take a moment to consider whether the main requirements of an adequate and relevant patient history taking have been fulfilled. Are there any additional questions you would have asked and, if so, why?
Before the physical examination findings are presented below, please reflect on what physical examination procedures you would perform to adequately evaluate this patient.
Performing Physical Examination
In the sections below, you are provided with examples of physical examination findings for this patient. The material presents a systematic approach to performing a focused and relevant physical examination in order to narrow down the possible causes for the patient’s complaint. The material also provides ongoing clinical reasoning and analysis of the findings. As you read the following material, you are encouraged to identify whether the essential elements of physical examination have been adequately covered.
Vital Signs
His vital signs are all within normal limits.
Analysis: It is always important to examine the vital signs to screen the patient’s general health and help identify underlying conditions such as infection.
Inspection
Evidence of mild swelling in the region of the fibular head is seen on inspection. There is no apparent bone deformity or bruising.
Analysis: Mild swelling confined to the region of the fibular head suggests several possible conditions including:
• Proximal tibiofibular joint sprain
• Biceps femoris tendinitis
• Lateral collateral ligament sprain
Range of Motion
He has a full range of motion on flexion and extension of the right knee but complains of some lateral knee discomfort at the extremes of both movements. The range of motion examination of the right hip reveals slight restriction in flexion when performed with the knee straight with the patient reporting tightness in the right posterolateral thigh. The lumbar spine range of motion is full and pain-free. The right ankle range of motion is normal but full passive dorsiflexion results in an aggravation of lateral knee pain. Resisted right knee flexion results in pain in the region of the fibular head.
Analysis: The findings on knee range of motion assessment simply confirm a mechanical problem in the lateral knee region whereas the result of the range of motion assessment for the hip suggests lateral hamstring involvement. The result of the ankle range of motion assessment suggests the involvement of the proximal tibiofibular joint. Pain on resisted knee flexion in the region of the fibular head suggests either involvement of the biceps femoris insertion or of the proximal tibiofibular joint.
Palpation
Mild swelling and moderate tenderness are found over the anterior and posterior aspects of the proximal tibiofibular joint. There is no tenderness over Gerdy’s tubercle or directly over the lateral margin of the tibiofemoral joint. There is tenderness on palpation of the distal portion of the biceps femoris tendon and its muscle belly feels hypertonic. Examination of the right proximal tibiofibular joint mobility elicits pain and reveals limited anterior glide of the proximal fibular head as compared to the left. Slight tenderness is also produced on palpation of the right ischial tuberosity and the sacroiliac joint.
Analysis: The mild swelling and tenderness directly over the proximal tibiofibular joint is strong evidence that this joint is involved. The lack of tenderness at Gerdy’s tubercle reduces the possibility of damage at the distal attachment of the iliotibial band. Tenderness and apparent hypertonicity of the biceps femoris implicate its involvement as well.
The loss of movement and pain on the attempted glide of the proximal tibiofibular joint further supports the involvement of this joint. Tenderness at the right ischial tuberosity and of the sacroiliac joint further supports the involvement of the biceps femoris and possibly sacroiliac joint dysfunction.
Reflection Point
Given the patient’s history and examination findings up until this point, please stop and take a moment to consider which special tests should be performed to further evaluate this patient.
Special Tests
To help rule out lateral meniscus involvement the McMurray’s test is performed and is found to be negative.
Analysis: The presence of lateral knee pain even in the absence of tibiofemoral joint locking or clicking warrants assessment for lateral meniscus injury. That the McMurray’s test is negative helps to rule out the involvement of the lateral meniscus. Please watch the video below if you wish to view how the McMurray’s test is performed.
The Ober’s and the Noble Compression tests are performed and both found to be negative.
Analysis: The negative results help to rule out the involvement of the iliotibial band. Please watch the videos below if you wish to view how these tests are performed.
The Varus Stress test for the knee is performed and found to be negative.
Analysis: The negative result helps to demonstrate the integrity of the lateral collateral ligament. Please watch the video below if you wish to view how the Varus Stress test is performed.
The Straight Leg Raise test is performed with the patient reporting discomfort in the posterior thigh and some aggravation of lateral knee pain on the right as the test approaches 90 degrees.
Analysis: The results are consistent with findings previously noted for ranges of motion assessment of the hip and suggest hypertonicity of the biceps femoris with either tendinopathy at its insertion or proximal tibiofibular joint involvement. Please watch the video below if you wish to view how the Straight Leg Raise test is performed.
The Gillet’s test is performed and demonstrates normal motion in both sacroiliac joints.
Analysis: The results suggest that the sacroiliac joints are unlikely to be involved. Please watch the video below if you wish to view how the Gillet’s test is performed.
Reflection Point
Please stop and take a moment to consider whether all the elements of an adequate and relevant physical examination have been completed for this patient. Are there any additional procedures you would have performed and, if so, why?
Imaging
Plain radiography of the knee is performed and reveals no evidence of fibular fracture or other bone pathology.
Clinical Diagnosis
Acute proximal tibiofibular joint dysfunction with associated biceps femoris hypertonicity.
Discussion
Mechanisms of injury for the proximal tibiofibular joint include direct impact trauma and forces arising out of twisting the lower leg or bending moments of the tibia. Aggravating factors for proximal tibiofibular joint sprain include injuries leading to dorsiflexion and eversion of the ankle, walking (particularly on uneven ground) and squatting. Some authors refer to biceps femoris hypertonicity as an associated finding which could cause a disturbance in the biomechanics of the pelvis and as a result leads to low back pain. The potential for irritation of the common peroneal nerve as it passes behind the swollen joint has also been suggested.
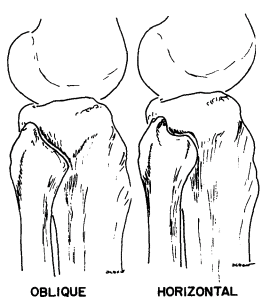
The proximal tibiofibular joint is described as a sliding synovial joint. In approximately 10% of cases, the joint capsule communicates with the tibiofemoral joint. Anatomical studies have revealed significant variations in the angle of the inclination of the proximal tibiofibular joint. Ogden classified the joint into two types as follows:
“The first type will be defined as horizontal. The fibular articular surface was usually planar (although it was slightly concave in some cases) and circular. The tibular surface articulated with a similarly planar, circular surface of the tibia. These articular surfaces were under and behind a projection of the lateral edge of the tibia) … The second type of proximal tibiofibular joint will be defined as oblique. The articular surfaces in this type were much more variable in surface area, configuration and inclination … The transition zone was chosen arbitrarily at 20°. The obliquity ranged all the way to 76°.”
With respect to the function of this joint, Ogden and other authors have noted that the fibula externally rotates with ankle dorsiflexion and that the fibular head slides forward with knee flexion (likely to be due relaxation of the lateral collateral ligament and biceps femoris) and slides backward with knee extension.
The clinical manifestations of proximal tibiofibular joint involvement include:
• Lateral knee pain (may radiate proximally and distally)
• Local swelling
• Hamstring tightness (particularly biceps femoris hypertonicity)
• Pain aggravation with knee and ankle movement (particularly dorsiflexion)
• Pain aggravation by resisted flexion of the knee
• Pain relieved by rest
• Painful fibular head on palpation
• Proximal tibiofibular joint motion palpation restriction
• Reduced knee extension due to hamstring tightness
References and Suggested Further Readings:
Bozkurt M. et al. The proximal tibiofibular joint: An anatomic study. Clinical Orthopaedics and Related Research. 2003, No 406, p. 136-140.
Ogden JA. The anatomy and function of the proximal tibiofibular joint. Clinical Orthopaedics and Related Research.1974, No 101, p. 186-191.
Radakovich M and Malone T. The superior tibiofibular joint: The forgotten joint. The Journal of Orthopaedic and Sports Physical Therapy. 1982, Vol 3, No 3, p. 129-132.
Beazell JR, Grindstaff TL, Magrum EM, Wilder R. Treatment of lateral knee pain by addressing tibiofibular hypomobility in a recreational runner. N Am J Sports Phys Ther. 2009;4(1):21–28.
Roxanne Caron. Mobilization Techniques for Proximal Tibiofibular Joint Dysfunction. Athletic Training and Sports Health Care. 2014;6(4):149-150
Travell JGb, Simons DG. Myofascial pain and dysfunction: The Trigger Point Manual. Baltimore: Williams and Wilkins.
Srbely JZ, Dickey JP, Lowerison M, Edwards AM, Nolet PS, Wong LL. Stimulation of myofascial trigger points with ultrasound induces segmental antinociceptive effects: A randomized controlled study. Pain. 2008 Oct 15;139(2):260–6.
Watson T. Ultrasound therapy. www.electrotherapy.org/modality/ultrasound-therapy
Watson T. Laser Therapy. www.electrotherapy.org/modality/laser-therapy
Baxter, D. (2008) Low Intensity Laser Therapy. Chapter 11 in : Electrotherapy : Evidence Based Practice.
Draper, D. O. et al. (2010). “Thermal ultrasound decreases tissue stiffness of trigger points in upper trapezius muscles.” Physiotherapy Theory and Practice 26(3): 167-172.
This concludes the learning material for this unit of the course.
Thank you for Reviewing this Free Sample.
This unit also has a multiple-choice quiz. The quiz is not included in this free sample.
Select Your Region Below to See All Approved Courses
Select Your Region Below
- United States
- Alaska
- Arizona
- California
- Colorado
- Connecticut
- Delaware
- District of Columbia
- Georgia
- Hawaii
- Idaho
- Illinois
- Indiana
- Iowa
- Kansas
- Kentucky
- Maine
- Maryland
- Massachusetts
- Michigan
- Minnesota
- Missouri
- Montana
- Nebraska
- Nevada
- New Hampshire
- New Jersey
- New York
- North Carolina
- North Dakota
- Ohio
- Oregon
- Pennsylvania
- Puerto Rico
- Rhode Island
- South Carolina
- South Dakota
- Texas
- Utah
- Vermont
- Virgin Islands
- Virginia
- Washington
- Wyoming
- Canada
- Other Countries
Disclaimer: The Chiropractic Online CE ™ website (including the text, graphics and videos that appear on the chiropracticonlinece.com) are designed to offer users general health information for educational purposes only. The general health information furnished on this site is not intended to replace personal consultation with a qualified healthcare professional. You must always seek the advice of a healthcare professional for questions related to your disease, disease symptoms, and appropriate therapeutic treatments.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.