
Free Sample – S1 Radiculopathy Caused by Disc Herniation: Diagnosis and Management (Preview)
Downloadable Patient Resources
For quick access, the links to the downloadable Practice Resource PDF files for this condition are available below.
Patient Information Sheet
Low Back Mobility Exercise Sheets
Core Strength Exercise Sheets
Please note:
The following sample material is from the course “Clinical Excellence in the Diagnosis and Treatment of Musculoskeletal Disorders- Volume 2”.
Disclaimer: Please read the Disclaimer at the bottom of this page.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.

Part 1: Diagnostic Features and Management
Classic Presentation
• Acute onset of low back pain.
• Pain involving the posterior thigh and leg that radiates into the lateral side of the foot (S1 nerve root pattern).
• Low back pain that eases after 24 hours with lower limb pain becoming predominant.
• Numbness and tingling (paresthesias) in the lower limb.
• Weakness in the leg.
• Pain aggravated by sitting, coughing, sneezing or straining.
Cause
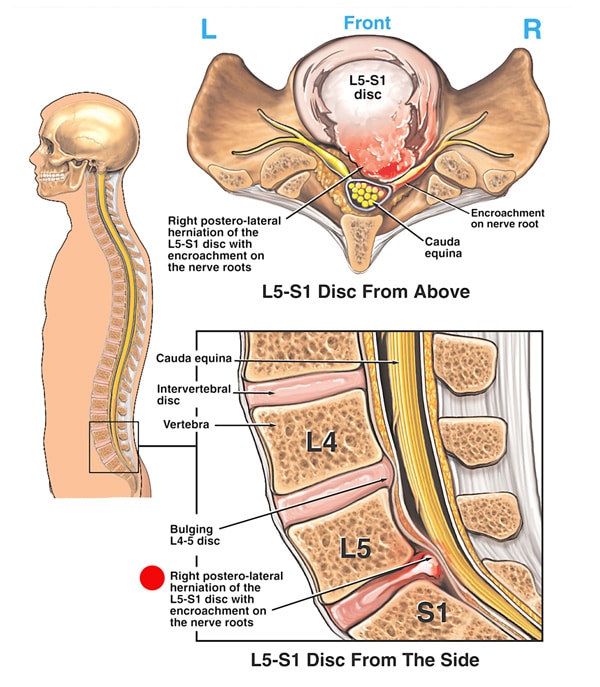
• Herniation of disc material leading to inflammation and/or compression of the nerve root.
• Disc herniation following heavy lifting, twisting or a straining injury.
Clinical Evaluation
• Weakness in ankle plantar flexion.
• Loss of sensation over the S1 dermatome, particularly the lateral heel.
• Reduced Achilles reflex.
• Positive sciatic nerve tension tests (e.g. Straight Leg Raise and Slump tests).
• Positive Valsalva test.
• Pain that is aggravated by lumbar flexion and reduced by lumbar extension.
Imaging
• Plain radiography to assess for osseous causes of radiculopathy (e.g, osteophytosis).
• MRI has advantages over CT. With MRI, there is no ionizing radiation and it is more sensitive in identifying other pathologies (e.g. inflammatory, malignancy and vascular conditions)
• CT enables better assessment of osseous structures than MRI and plain radiography. However, it is unable to sufficiently demonstrate the nerve root.
Red Flags
The following are examples of red flags for patients presenting with low back pain and lower extremity symptoms:
• Gradual onset of signs and symptoms of radiculopathy.
• Worsening radiculopathy signs and symptoms.
• History of significant trauma.
• Bilateral lower extremity symptoms.
• Pronounced neurological impairment.
• Bladder and bowel dysfunction.
• Saddle anesthesia.
• Severe tenderness on palpation or severe pain with any examination procedure.
• Unexplained weight loss
If any red flags are identified during history taking and clinical examination, referral for urgent medical evaluation and further investigation is warranted.
When the Patient’s Evaluation Reveals Red Flags
When “red flags” are identified, serious conditions including infection, fracture, dislocation or tumors need to be ruled out before any treatment can commence.
• Refer for medical evaluation and further investigation.
• See a sample referral letter below. You are encouraged to include more information in the letter if required (e.g. the suspected diagnosis or a list of differentials for the patient).
[Date]
[Medical Practitioner’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
Thank you for seeing [Patient’s Name] who presented at my clinic today with the following clinical history and examination findings: [specify – below are some examples]
• A history of severe trauma
• Severe low back pain radiating to the right/left lower extremity
• Unrelenting and/or nocturnal pain
• Low back pain and urinary incontinence
• Bilateral sciatica
• Extensive bruising in the lower back
• Swelling, warmth and restricted movement at the lumbosacral region
• Back pain and fever
I have discussed my concerns regarding the above findings with the patient and have recommended that they see you for a medical evaluation immediately.
I would be grateful if, with [Patient’s Name]’s consent, you would inform me of the results of your assessment and investigation.
Thank you for your evaluation please do not hesitate to contact me if you require further information.
Yours sincerely,
[Your Name]
[Your Qualifications]
Patient Management
If no red flags are identified or further investigations do not reveal any contraindications to treatment, management of the condition may begin.
Purpose
The overall purpose of treatment and rehabilitation is to return the patient to preinjury status as soon as possible. As such, the patient’s management plan needs to include the required elements of an effective therapeutic and rehabilitation program.
Goals
• To eliminate pain
• To restore function
• To rehabilitate the region and provide advice to prevent reinjury

For a faster patient recovery, we advocate a management approach that includes all of the following components:
• A gentle correction of joint dysfunction
• The inclusion of soft tissue therapy
• The provision of support and home advice
• The inclusion of rehabilitation exercises
Please Note: The management approach outlined below is based on published materials (see the References section at the end of this web page) and the clinical experience of the authors of this course. This should not be interpreted as a prescriptive guide to the treatment of this or any other condition. The use of this content is subject to the Disclaimer found at the bottom of this web page.
Treatment and Home Advice
Caution: In the case of severe low back pain and sciatica, at every consultation, the patient’s clinical signs and symptoms should be carefully monitored to ensure that there is no deterioration. In the case of deterioration, referral for CT or MRI of the lumbosacral spine is required.
Correction of Joint Dysfunction
• Evaluation and correction of any dysfunctional joints (if present) in the sacroiliac and lumbar regions.
• Any management techniques that are applied should minimize excessive loading at the level of the disc herniation.
• It is recommended that, when targeting the level of disc herniation, handheld instrument-assisted procedures or traction are utilized. Some authors indicate that manual spinal manipulation for the level of involvement can be considered, but they stress that this must be performed cautiously and with no or minimal spinal rotation.
McKenzie Method
Consider applying the “McKenzie Method” for discogenic pain.
Soft Tissue Therapy
Electrotherapy: Some patients benefit from the application of ultrasound phonophoresis and/or low-level laser to assist with pain reduction and soft tissue healing.
Myofascial Release: The application of trigger point therapy or other soft tissue procedures for the spine and pelvic musculature as indicated.
The application of ice for pain management.
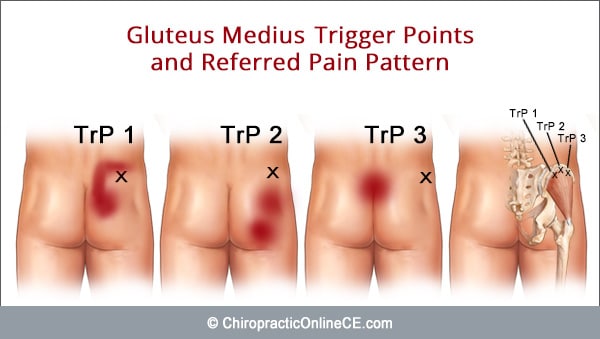
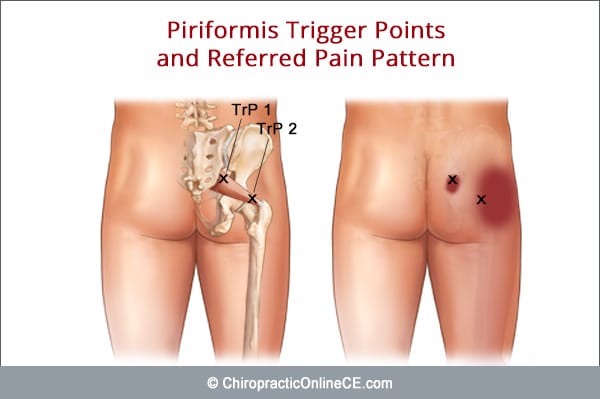
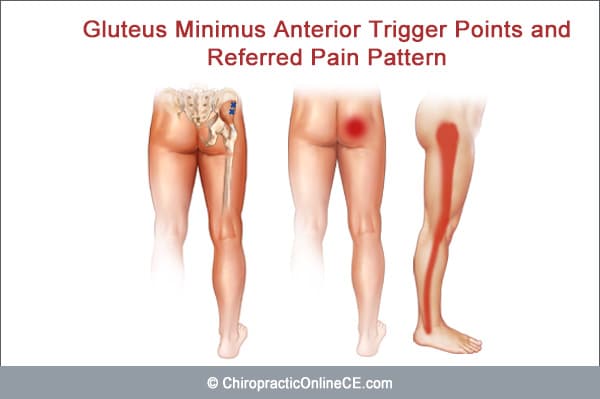
In patients presenting with low back and leg pain, a complete clinical examination should include evaluation of the following muscles to check for the presence of myofascial trigger points as concomitant or the primary causes of the patient’s pain:
• Gluteus medius
• Piriformis
• Gluteus minimus
Support
The application of taping if required.
Home Advice
Ask the patient to:
• Apply ice over the affected region for about 10 minutes, several times a day for pain control. Ice can be applied as often as every hour.
• Wear a suitable lumbopelvic brace for only a few days (wear it intermittently)
• Avoid any aggravating activities (e.g. bending forward, prolonged sitting and standing).
• Sit down on a chair or a bed when removing or putting on trousers
Some practitioners advocate the use of moist heat in the subacute or chronic phase. However, we have found that patients often benefit from the continued application of ice to reduce discomfort as they engage in more activities to restore a full and pain-free spinal function.
Additional Pain Management
Refer the patient for medical co-management when additional pain reduction strategies are required.
Patient Information
Patient Information
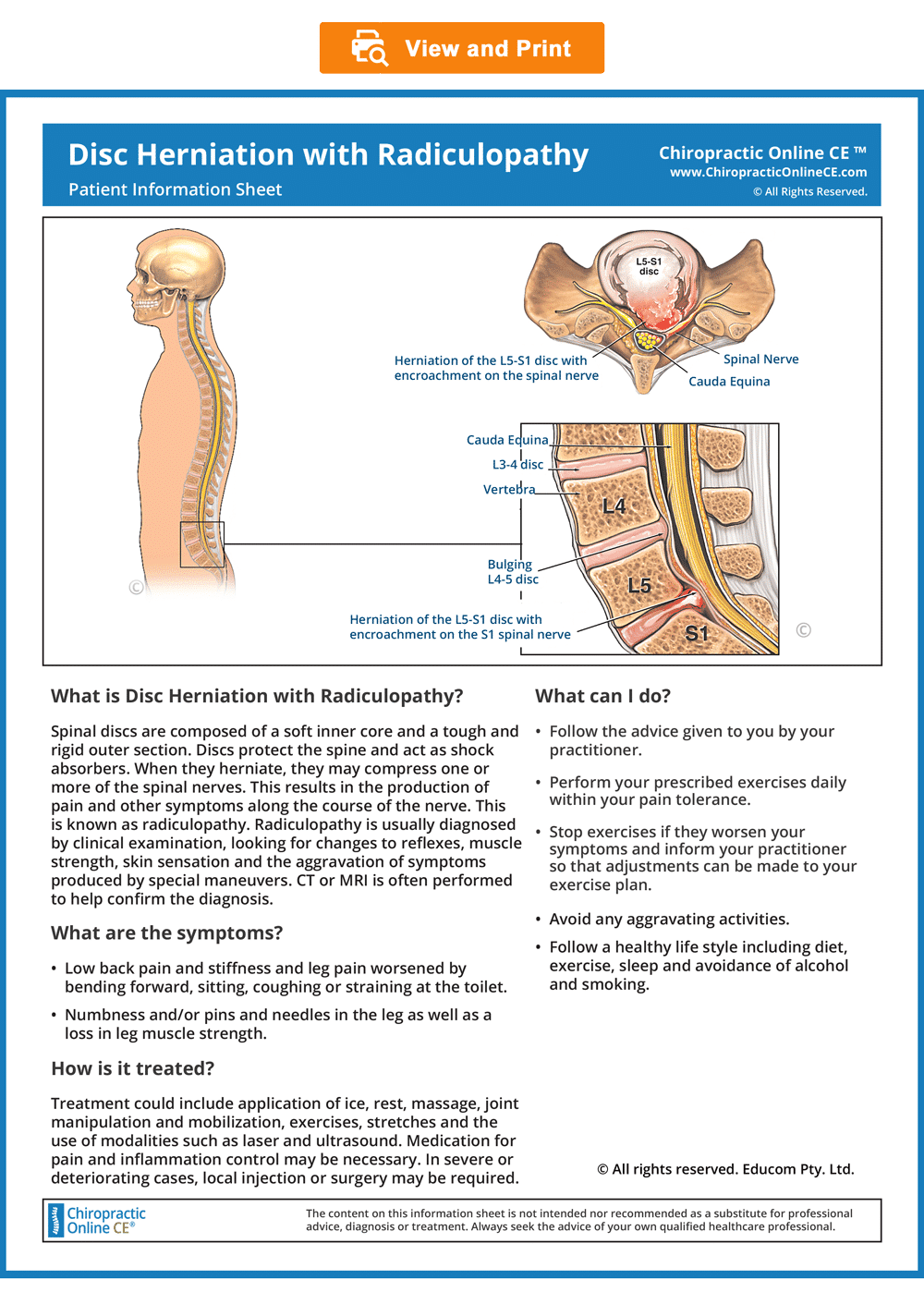
Provide information to the patient about the condition to improve their understanding of the condition and enhance compliance (see the downloadable ready-to-use Patient Information Sheet below).
Please note that the bottom right-hand corner of the Patient Information Sheet has been intentionally left blank to allow you to attach your business card.
We encourage our patients to show the information sheets to their family, friends and their medical practitioner, all leading to new patient referrals.
To view, download or print the Patient information sheet, simply click on the image below.
Patient Information Sheet
© Educom Pty. Ltd. All Rights Reserved.
Exercise Prescription
General Principles of Exercise Prescription
• When appropriate, the patient should gradually begin doing exercises at home.
• Always recommend warm-up activities before commencing specific exercises. Warm-up activities include simple limbering movements or prescribed strength exercises at light loads.
• Instruct your patients to perform any strengthening exercises before they perform any stretching exercises.
• Always instruct your patients to use caution when performing their rehab exercises in order to avoid overloading, overstretching or any undue pain.
• Emphasize that they should stop any exercises that cause them concern and seek your advice at the earliest opportunity.
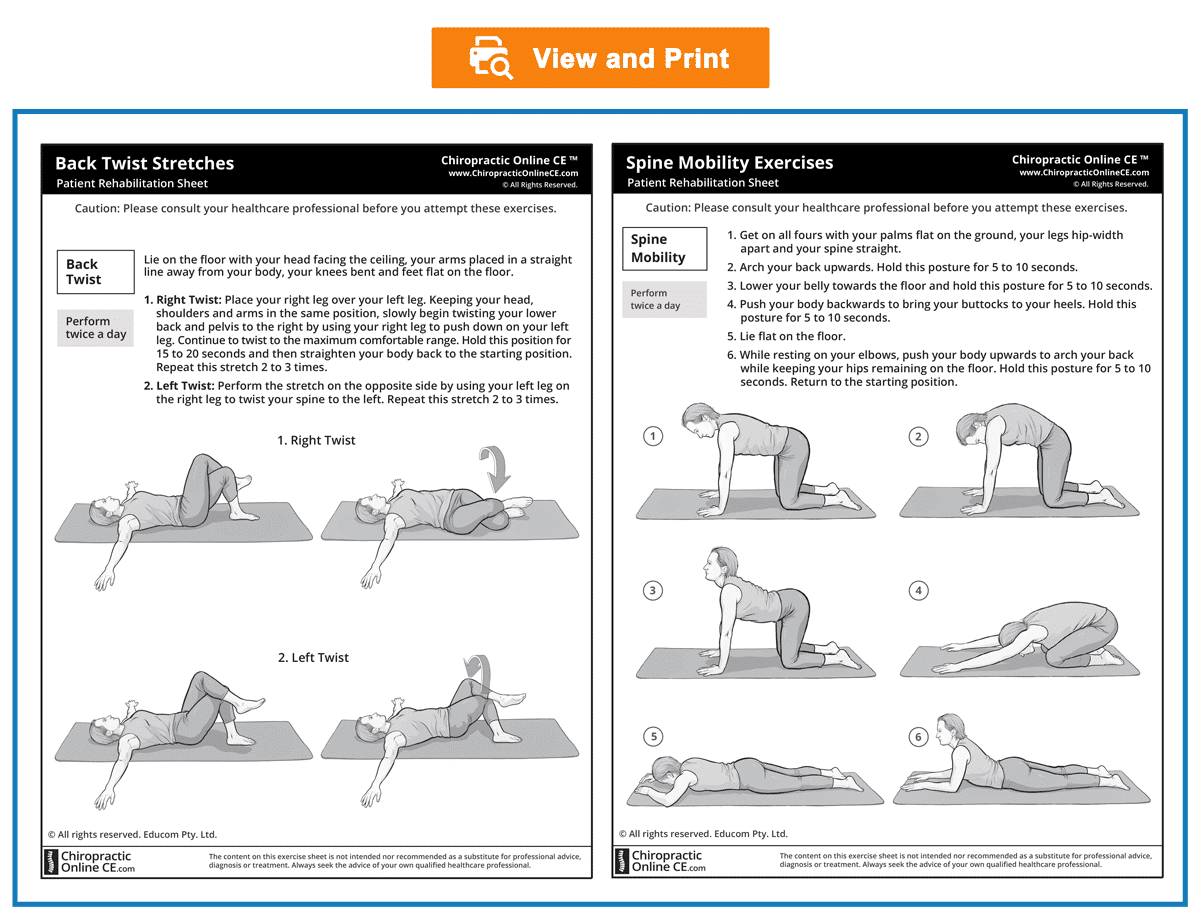
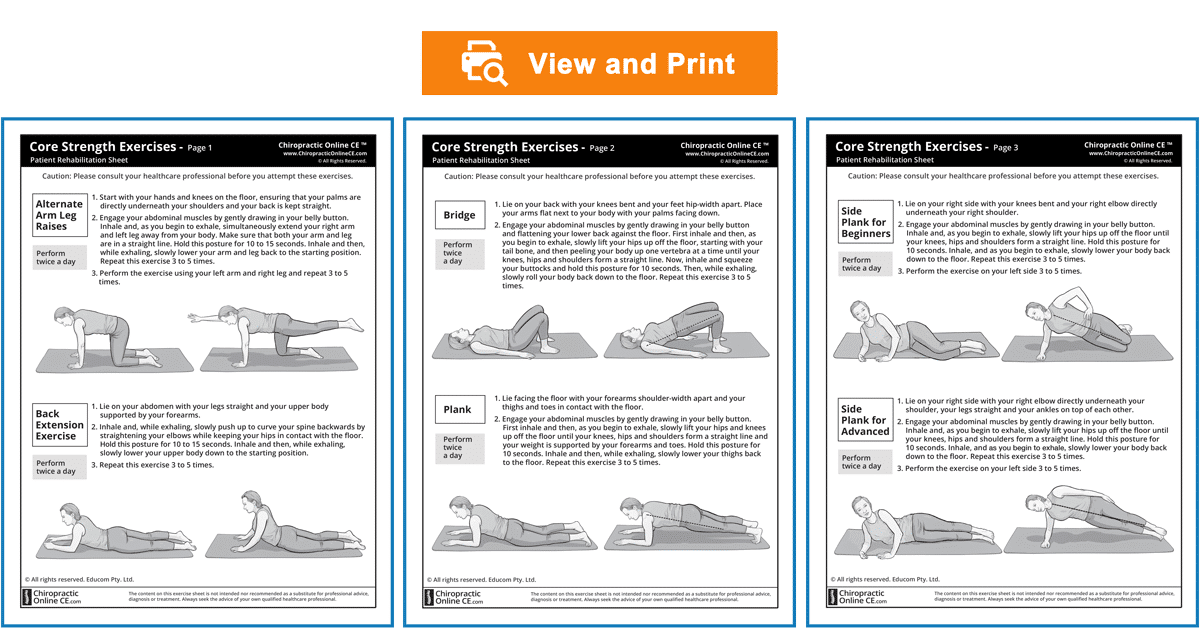
Provide rehabilitation exercise sheets to your patients (see the downloadable ready-to-use Rehabilitation Sheets below).
Download and print out the rehabilitation exercise sheets.
Choose the exercises that you consider to be most appropriate for your patient’s stage of recovery and strike out those that are not required.
We encourage our patients to show their exercise sheets to their family, friends and even their medical practitioner, all leading to new patient referrals.
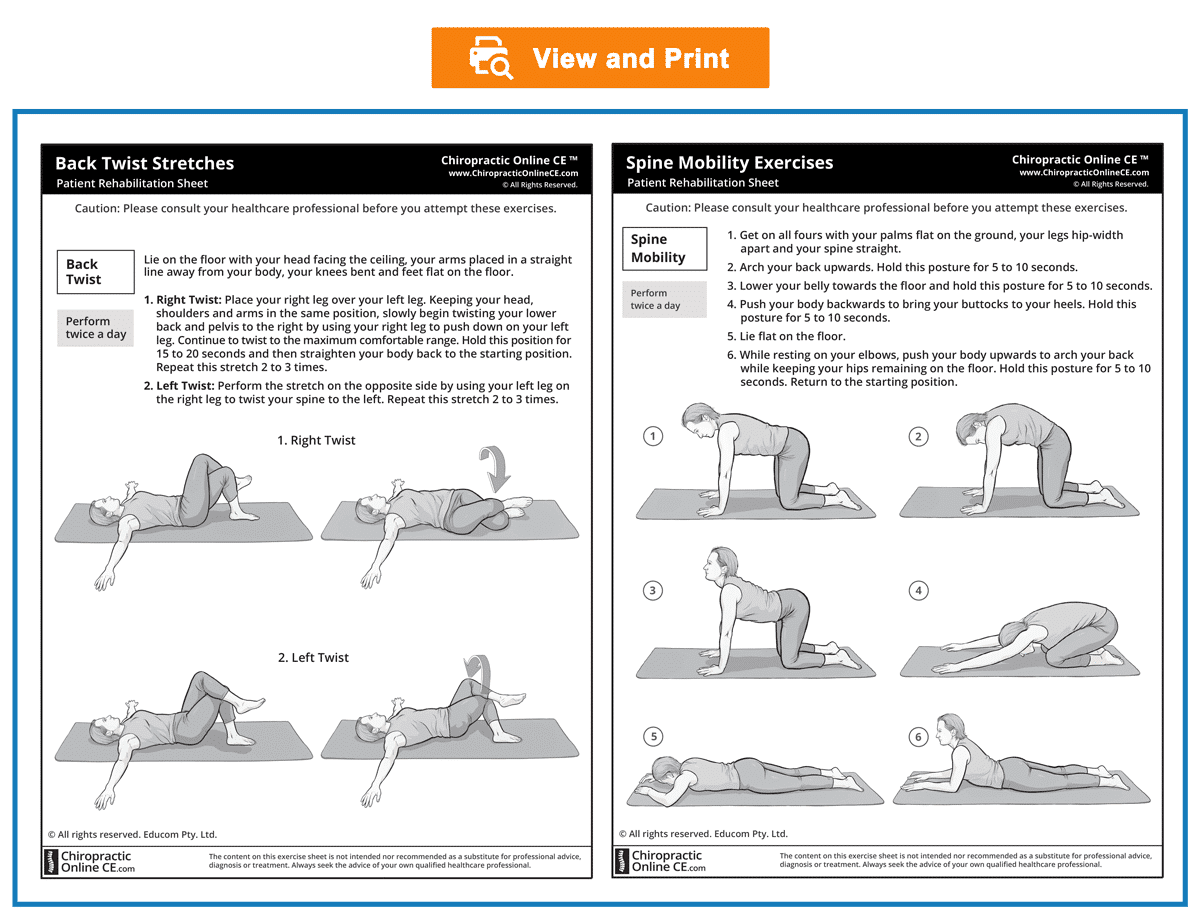
Low Back Mobility Exercises
© Educom Pty. Ltd. All Rights Reserved.
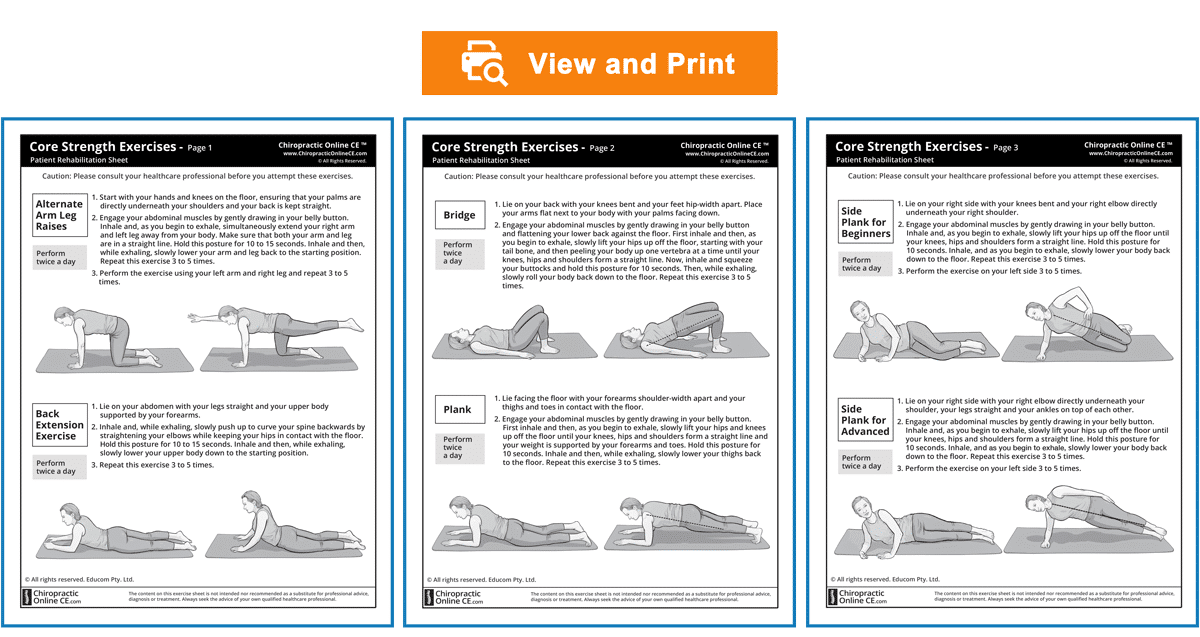
Core Strength Exercises
© Educom Pty. Ltd. All Rights Reserved.
Courtesy Letter to the Patient’s Medical Practitioner
Writing a letter to your patient’s medical practitioner (with the patient’s consent) to advise them that you have commenced treatment for the patient helps to demonstrate your professional knowledge, clinical skills and willingness to collaborate with the medical practitioner in caring for the patient. This approach is effective in improving awareness of the range of treatment modalities you can provide at your practice and could encourage the medical practitioner to refer new patients to your practice.
You will see a sample referral letter below. You are encouraged to include more information in the letter if required (e.g. case history, examination findings and the full management plan).
[Date]
[Doctor’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
I am writing to advise you that [Patient’s Name] has presented at my clinic with low back and [side] lower extremity pain which I have diagnosed as disc herniation with radiculopathy. [Patient’s Name] advised me that you are their medical practitioner and has provided consent for me to contact you.
I have commenced a management plan that includes a gentle adjustive procedure to improve spinal alignment and function as well as myofascial release and therapeutic ultrasound to facilitate soft tissue recovery. I have also provided the patient with an information sheet about the condition to increase compliance and rehabilitation exercise sheets to hasten recovery and help prevent re-injury. Copies of these resources are attached to this letter for your reference.
Please do not hesitate to contact me if you require further information or have any suggestions.
Yours sincerely,
[Your Name]
[Your Qualifications]
If the Patient is Not Responding to Treatment
If the patient is not responding to treatment:
• Re-evaluate the patient’s clinical presentation.
• If an alternate disorder that is within your scope of practice is uncovered, manage appropriately. If not, refer the patient for further evaluation.
• See a sample referral letter below. You are encouraged to also include the date of the first presentation, case history and examination findings that led you to your diagnosis).
[Date]
[Medical Practitioner’s Name and Address]
Re: [Patient’s Name] – Date of Birth: [Patient’s Date of Birth]
Dear Dr. [Doctor’s Name],
Thank you for seeing [Patient’s Name] who presented at my clinic with low back and [side] lower extremity pain which I have diagnosed as disc herniation with radiculopathy. I implemented a management plan that included a gentle adjustive procedure to improve spinal alignment and function, myofascial release and therapeutic ultrasound, and rehabilitation exercises. The patient’s response has been unsatisfactory to date and therefore I am referring them to you for your evaluation and consideration.
Thank you for evaluating the patient and please do not hesitate to contact me if you require further information.
Yours sincerely,
[Your Name]
[Your Qualifications]
S1 Radiculopathy Caused By Disc Herniation
Part 2: Clinical Case Scenario
Please read the following material and watch the videos.
A Problem-Solving Approach to History Taking and Physical Examination
The learning material in this unit is designed to improve your skills in history taking and physical examination. The material includes examples of clinical findings and their analysis using a problem-solving approach. As you read through the material and watch the videos, you are encouraged to identify whether all the required elements of history taking and physical examination have been adequately covered.
Patient’s History
Read the following case scenario to refresh and improve your clinical reasoning when taking the patient’s case history. When taking the patient’s history, the practitioner needs to obtain sufficient information to cover the following essential elements.
Who is the patient and where is the pain?
When was the onset and what caused the onset?
Your patient is a 38-year-old fitter and turner who presents with a primary complaint of low back and lower extremity pain. He points to the right side of his lower lumbar region, right posterior thigh and leg as the main sites of his pain. He says that his low back pain started 3 days ago after lifting heavy machinery at work. Within 24 hours, his back had become stiff, resulting in very limited movement.
Analysis: This is a case of a patient with acute back pain due to a recent work-related incident. His occupation makes him vulnerable to mechanical conditions of the lumbar spine. Pain in the lower lumbar region and lower extremities is common and can indicate a number of conditions, including:
• Vertebral motion segment dysfunction
• Sacroiliac joint dysfunction
• Myofascial pain syndromes (e.g. piriformis trigger point referral)
• Muscle strain (e.g. the erector spinae muscle)
• Disc injury
• Piriformis syndrome
He says that his right lower extremity pain developed the day after the onset of the low back pain and has gradually worsened while the low back pain has eased.
Analysis: The development of right lower extremity symptoms within 24 hours of the onset of low back pain suggests a causal relationship. Lumbar disc herniation typically presents with low back pain and begins to abate after the first 24 hours while radiculopathy develops and becomes predominant.
What are the pain characteristics?
What are the aggravating and relieving factors?
What has been the course of the pain?
He says that, in the beginning, his low back pain felt like he was being stabbed and was a 10 out of 10 in intensity. However, he says that his lower back feels better now and has reduced to a 6 out of 10. He says that the stiffness in his back has persisted since the onset. He describes the right posterior thigh and leg pain as an intense “burning”. This pain is most pronounced in his calf. His lower extremity pain varies in intensity but he rates it as an 8 out of 10 when at its most severe. The patient reports an increase in his low back and lower extremity pain when he coughs or sneezes. The pain also worsens if he sits for long periods of time. He indicates that resting in bed causes the pain to ease off but it does not completely disappear.
Analysis: The persistence of his lower extremity symptoms with a reduction of his low back pain correlates well with the natural history of intervertebral disc herniation causing radiculopathy. His description of a burning-type pain suggests a neurological cause and strengthens the possibility of a disc lesion. The distribution of his posterior thigh and leg pain is consistent with low lumbar radiculopathy. The aggravation of his pain with prolonged sitting and with coughing and sneezing are commonly reported by patients suffering from radiculopathy due to space-occupying lesions such as disc herniation.
Are there any associated symptoms?
He reports that, for several months, he has been aware of a vague tingling sensation in his right calf.
Analysis: The presence of a tingling sensation in his right lower extremity suggests neurological impairment. That it has been present for several months prior to the onset of his low back and lower extremity pain indicates that the underlying condition may have been evolving for some time.
Is there a past history that is relevant to the current complaint?
His past history reveals several episodes of low back pain but these have never prevented him from working and always resolved quite quickly. He says that his current pain is more severe than ever before and he has been off work since it began. He admits to being a heavy smoker.
Analysis: The patient’s occupational demands and smoking habit are predisposing factors that increase the risk of spinal injuries including intervertebral disc herniation. The fact that his current pain is more severe than previous episodes may indicate that the condition is deteriorating or that there is a new underlying disorder.
Are there any “red flags”?
The patient is asked the following questions in order to identify any “red flags” that could indicate serious pathology. Even if the patient has already provided information in the case history that relates to these questions, it is recommended that they are readdressed to ensure a thorough exploration.
Do your symptoms disappear even for a short time? “Not really, but the symptoms do ease when I am in bed.”
Does the pain wake you up at night? “It does not wake me up, but if I wake up in the middle of the night I notice that the pain is still there.”
Have you noticed any discoloration of your urine? “No.”
Have you had any bladder or bowel problems since the onset of your pain? “No.”
Do you feel weak in your legs? “Yes. My right leg feels weaker, especially when I’m climbing stairs.”
Have you recently experienced any fever, chills, night sweats or vomiting? “No”.
Have you lost any weight recently? “No.”
Do you have a history of cancer or HIV? “No.”
Analysis: The persistence of his pain, together with the perceived weakness of his right leg, raise red flags. However, these findings can be due to a mechanical disorder such as nerve root compression due to disc herniation.
What is the list of possible causes for the patient’s complaint?
Based on the available history, several conditions could be involved and will need to be explored during the physical examination. These include:
• Lumbar disc herniation or other space-occupying lesion causing radiculopathy
• Piriformis syndrome
• Vertebral motion segment dysfunction
• Sacroiliac joint dysfunction
Reflection Point
Please stop and take a moment to consider whether the main requirements of an adequate and relevant patient history taking have been fulfilled. Are there any additional questions you would have asked and, if so, why?
Before the physical examination findings are presented below, please reflect on what physical examination procedures you would perform to adequately evaluate this patient.
Performing Physical Examination
In the sections below, you are provided with examples of physical examination findings for this patient. The material presents a systematic approach to performing a focused and relevant physical examination in order to narrow down the possible causes for the patient’s complaint. The material also provides ongoing clinical reasoning and analysis of the findings. As you read the following material, you are encouraged to identify whether the essential elements of physical examination have been adequately covered.
Vital Signs
His vital signs are within normal limits.
Analysis: It is always important to examine the patient’s vital signs to screen for general health and identify any underlying conditions such as an infection.
Inspection
The patient is unable to fully stand up straight and leans slightly to the left. Local inspection of the back shows a flattening of the lumbar curve.
Analysis: The patient’s inability to straighten up and his leaning to the left away from the side of the lower extremity pain suggest an antalgic posture. These findings are typically associated with posterolateral disc herniation causing radiculopathy. Flattening of the lumbar lordosis can also be due to muscle guarding and is often seen in acute disc herniation.
Range of Motion
The active lumbar ranges of motion are reduced in all directions. Flexion and lateral flexion toward the right side both aggravate his lower extremity symptoms.
Analysis: The loss of all active ranges of motion is consistent with a mechanical cause for his low back pain due to protective muscle hypertonicity. The aggravation of his lower extremity symptoms on flexion and lateral flexion toward the painful side suggests posterolateral disc herniation and nerve root entrapment.
Palpation
Palpation of the lumbar spine reveals local tenderness over the L5 spinous process and in the interspace between the L5 spinous process and S1 sacral tubercle. When firm pressure is applied over the same interspace, the patient reports an aggravation of burning and tingling in the right posterior calf. Palpation of the right sacroiliac joint reveals local tenderness but without pain referral. Pressure applied midway between the sacrum and the right greater trochanter results in a slight aggravation of the patient’s lower extremity symptoms.
Analysis: The palpation findings help to strengthen the likelihood of a local mechanical cause for the patient’s back pain. That pressure applied to an interspinous space results in the exacerbation of his radicular symptoms indicates a positive Bell test suggesting a disc lesion causing radiculopathy. In this patient, it suggests an L5 disc lesion involving the S1 nerve root. The tenderness found over the right sacroiliac joint indicates that further examination of this joint is warranted. The slight aggravation of the lower extremity symptoms with pressure applied to the gluteal region reinforces sciatic involvement.
Neurological Examination
A neurological examination for the low back region is performed and reveals the following:
• Significant loss of strength of right ankle plantar flexion
• Loss of sensation over the right lateral heel
• No loss of sensation in the “saddle” region
• Reduced right Achilles reflex
• Absence of Babinski response
• No evidence of ankle clonus
Analysis: These findings are consistent with right S1 nerve root involvement. Please watch the videos below if you wish to view how a Neurological Examination for the low back region may be performed.
Reflection Point
Given the patient’s history and examination findings up until this point, please stop and take a moment to consider which special tests should be performed to further evaluate this patient.
Special Tests
The Valsalva test is performed and is found to aggravate the symptoms of his right lower extremity.
Analysis: A positive Valsalva test is further evidence of nerve root compromise due to a space-occupying lesion such as a herniated disc. Please watch the video below if you wish to view how the Valsalva test is performed.
The Slump test is performed and is also found to aggravate the symptoms of his right lower extremity.
Analysis: A positive Slump test is further evidence of lumbar disc herniation causing radiculopathy. Please watch the video below if you wish to view how the Slump test is performed.
The Straight Leg Raise (SLR) test is performed and causes aggravation of the symptoms of his right lower extremity. The test is repeated with ankle dorsiflexion (Bragard’s test) and cervical spine flexion, with both reproducing the patient’s right lower extremity symptomatology.
Analysis: The positive SLR test, together with a positive response to ankle dorsiflexion and cervical flexion, all strongly indicate radiculopathy. Please watch the video below if you wish to view how the SLR test is performed.
The Well Leg Raise (WLR) test is performed on the left side and causes slight aggravation of the symptoms of his right lower extremity.
Analysis: A positive WLR test helps to confirm the presence of sciatic radiculopathy. Please watch the video below if you wish to view how the Well Leg Raise test is performed.
The Piriformis test is performed and does not aggravate the symptoms of his lower extremity.
Analysis: A negative Piriformis test helps to rule out sciatic neuropathy arising from piriformis syndrome. Please watch the video below if you wish to view how the Piriformis test is performed.
Reflection Point
Please stop and take a moment to consider whether all the elements of an adequate and relevant physical examination have been completed for this patient. Are there any additional procedures you would have performed and, if so, why?
Imaging
The patient is referred for Magnetic Resonance Imaging. The report indicates the presence of a moderate right posterolateral disc herniation at the L5-S1 level with S1 nerve root encroachment.
Clinical Diagnosis
Right posterolateral disc herniation at the L5-S1 level with S1 radiculopathy
Discussion
Lumbar Disc Herniation with Radiculopathy
The North American Spine Society defines lumbar disc herniation with radiculopathy as “. . . localized displacement of disc material beyond the normal margins of the intervertebral disc space resulting in pain, weakness or numbness in a myotomal or dermatomal distribution.”
With regard to the gold standard for diagnosis of lumbar disc herniation the Society states:
“Cross-sectional imaging exams have a low intrinsic specificity as evidenced by a significant incidence of pathologic findings in asymptomatic populations. The results of any cross-sectional examination need to be closely correlated with the clinical examination. As a result, the accuracy of a spine MRI or CT should incorporate the ability of the test to directly visualize neurologic structures and the effect of pathologic processes on these structures. Direct visualization of intrinsic neurologic processes and neural impingement is of obvious importance in determining the etiology of radicular symptoms.
The gold standard in the majority of the studies confirming the presence of a herniated disc was cross-sectional imaging and/or surgery. The gold standard in the diagnosis of lumbar disc herniation is surgery; however, when assessing the validity of subjective complaints or physical examination findings, use of cross-sectional imaging as a gold standard may be considered an acceptable substitute. The validity of surgery as a gold standard can be questioned, however, as findings at surgery can be subjective”.
There are a number of special tests designed to detect the presence of radiculopathy. The supine Straight Leg Raise test is considered to be the most sensitive for low lumbar nerve root involvement. However, this test lacks specificity and therefore cannot be relied upon on its own.
Lumbar disc herniation with subsequent radiculopathy most typically involves the L4-L5 and L5-S1 levels. Disc herniation is less common in the upper lumbar region. For example, the incidence of L3-L4 herniation is approximately one-tenth that of the incidence of L5-S1 herniation.
References and Suggested Further Readings:
Jenkins A, Ahuja A, Oliff A, Sobotka S. Spinal Schwannoma Presenting Due to Torsion and Hemorrhage: Case Report and Review of Literature. Spine J. 2015 Aug 1;15(8)
Tawa N, Rhoda A, Diener I. Accuracy of clinical neurological examination in diagnosing lumbo-sacral radiculopathy: a systematic literature review. BMC Musculoskelet Disord. 2017 Feb 23;18(1):93.
van der Windt D, Simons E, Riphagen I, Ammendolia C, Verhagen A, Laslett M, Devillé W, Deyo R, Bouter L, de Vet H, Aertgeerts B. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 2010 Feb 17;(2):CD007431
Clinical Guidelines for Multidisciplinary Spine Care. Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy. North American Spine Society (2012)
www.uptodate.com
Travell JGb, Simons DG. Myofascial pain and dysfunction: The Trigger Point Manual. Baltimore: Williams and Wilkins.
Srbely JZ, Dickey JP, Lowerison M, Edwards AM, Nolet PS, Wong LL. Stimulation of myofascial trigger points with ultrasound induces segmental antinociceptive effects: A randomized controlled study. Pain. 2008 Oct 15;139(2):260–6.
Watson T. Ultrasound therapy. www.electrotherapy.org/modality/ultrasound-therapy
Watson T. Laser Therapy. www.electrotherapy.org/modality/laser-therapy
Baxter, D. (2008) Low Intensity Laser Therapy. Chapter 11 in : Electrotherapy : Evidence Based Practice.
Draper, D. O. et al. (2010). “Thermal ultrasound decreases tissue stiffness of trigger points in upper trapezius muscles.” Physiotherapy Theory and Practice 26(3): 167-172.
This concludes the learning material for this unit of the course.
Thank you for Reviewing this Free Sample.
This unit also has a multiple-choice quiz. The quiz is not included in this free sample.
Select Your Region Below to See All Approved Courses
Select Your Region Below
- United States
- Alaska
- Arizona
- California
- Colorado
- Connecticut
- Delaware
- District of Columbia
- Georgia
- Hawaii
- Idaho
- Illinois
- Indiana
- Iowa
- Kansas
- Kentucky
- Maine
- Maryland
- Massachusetts
- Michigan
- Minnesota
- Missouri
- Montana
- Nebraska
- Nevada
- New Hampshire
- New Jersey
- New York
- North Carolina
- North Dakota
- Ohio
- Oregon
- Pennsylvania
- Puerto Rico
- Rhode Island
- South Carolina
- South Dakota
- Texas
- Utah
- Vermont
- Virgin Islands
- Virginia
- Washington
- Wyoming
- Canada
- Other Countries
Disclaimer: The Chiropractic Online CE ™ website (including the text, graphics and videos that appear on the chiropracticonlinece.com) are designed to offer users general health information for educational purposes only. The general health information furnished on this site is not intended to replace personal consultation with a qualified healthcare professional. You must always seek the advice of a healthcare professional for questions related to your disease, disease symptoms, and appropriate therapeutic treatments.
Copyright © Educom Pty Ltd: All material on this website (including the text, graphics, videos and downloadable files) are owned by or licensed to Educom Pty Ltd and is subject to copyright and other intellectual property rights under international conventions.